
RSM Blog: Manual Therapy Techniques
Exploring the Clinical Benefits of Trigger Point Massage Therapy

Trigger Point Massage Therapy for chronic pain
Localized tenderness within muscle tissue often signals the presence of a myofascial trigger point. These hyperirritable spots, located in a taut band of skeletal muscle, produce pain locally and in referred patterns. In RSM's Trigger Point Therapy Course, we teach that understanding these physiological anomalies is the foundation of effective sports medicine.
My experience has shown that ignoring these points leads to a cascade of dysfunction. A single untreated nodule alters muscle function, creating compensation patterns. We emphasize to our students that effective treatment requires precision. It is not enough to apply general pressure; a therapist must understand the pathology to facilitate true healing.
Defining the Trigger Mechanism in Muscle Pain
A trigger point is essentially a microscopic cramp. At the cellular level, sarcomeres remain locked in a contracted state. This restricts blood flow to the area, causing a buildup of metabolic waste. This toxic environment sensitizes nerve endings, creating the sharp pain often described by patients.
We categorize these into active and latent types. Active points cause discomfort spontaneously. Latent points only generate sensation when compressed, yet they still restrict movement. Identifying these hidden areas is a critical skill for any massage therapist.
Addressing Chronic Pain through Targeted Massage
Chronic pain often stems from untreated myofascial dysfunction. Conventional approaches may fail if they address symptoms rather than sources. Massage techniques designed for these points focus on interrupting the pain-spasm cycle.
We utilize ischemic compression. The therapist applies sustained pressure to the nodule, temporarily cutting off blood supply. Releasing the pressure causes fresh, oxygenated blood to rush in—a process called reactive hyperemia. This flushes out toxins. Reduced pain is the immediate result. For chronic conditions like tension headaches, this interruption of neural signals resets the neuromuscular junction.
Enhancing Circulation via Triggerpoint Therapy
Triggerpoint therapy systematically improves vascular efficiency. Tense bands caused by these points act like dams, obstructing blood and lymph flow. This stagnation prevents tissue from healing after exertion.
By releasing the constriction, we restore proper hemodynamics. Improved circulation ensures repair cells reach damaged fibers. We observe that patients receiving this specific therapy report higher energy levels because the metabolic burden decreases. The heart no longer fights against the resistance of tight muscles to pump blood.
Reducing Pain and Restoring Function
One of the most complex aspects of musculoskeletal dysfunction is referred pain. This occurs when the source of discomfort is distant from where the patient feels it. For example, a knot in the gluteus may mimic sciatica. Treating the source eliminates the ghost symptom, leading to substantial pain relief.
Restoring function involves mechanics. A muscle shortened by a trigger point cannot stretch to its full length, limiting the joint’s range of motion. Release of the trigger point restores the length-tension relationship. The joint regains its freedom, allowing the athlete to move with efficiency.
Integrating Modalities for Optimal Results
The body functions as a tensegrity structure. Trigger point therapy works best as part of a comprehensive plan. We often integrate it with chiropractic adjustments or movement re-education. Musculoskeletal pain involves nerves, fascia, and joints. A single-mode approach often yields limited results.
By combining specific point therapy with other modalities, we ensure long-term success. Patients with back pain often find that a combination of release work and corrective exercise solves persistent issues. The release provides the window of opportunity; the exercise builds the strength to maintain it.
Recognizing the Signs
It is essential to recognize when specific points require attention. If a patient presents with tightly wound areas or discomfort that does not respond to stretching, trigger point involvement is likely. Stretching an active knot can aggravate the spasm by triggering a stretch reflex.
We prioritize release before elongation. We must disengage the spasm before attempting to lengthen the fiber. This sequence is non-negotiable in our clinical practice.
Clinical Efficacy
The benefits of trigger point therapy extend beyond temporary relief. This modality addresses the physiological root of dysfunction. At RSM International Academy, this is a fundamental component of sports medicine. By mastering trigger point therapy and targeted point therapy, we unlock the body’s potential. We allow patients to move without restriction. This is the core of our mission.
Mastering Remedial Massage Assessment Methods

Remedial Massage Course Chiang Mai
Correct diagnosis is the distinction between temporary relief and long-term recovery. In the elite sports medicine circles where I operate, we frequently encounter practitioners who rush immediately into treatment without understanding the biomechanical root of the problem. This approach is akin to a mechanic replacing a tire when the axle is bent; the symptom may vanish momentarily, but the dysfunction persists.
In the Remedial Massage Course at RSM International Academy, I teach that treatment begins the moment the individual enters the room. Before we apply any oil, we must gather data. We act as investigators, piecing together clues from movement patterns, tissue texture, and verbal history. Only then can we construct a strategy that addresses the source of the issue rather than merely silencing the pain.
The Critical Role of Massage Therapists in Clinical Analysis
Entry-level courses often frame massage primarily as a relaxation tool. While relaxation is a valid outcome, it is not the primary objective of clinical rehabilitation. Massage therapists aiming for the top tier of the industry must possess the skills to evaluate clients’ musculoskeletal health with precision. This shift in mindset transforms the practitioner from a simple service provider into a vital member of the client’s healthcare team.
When we approach a bodywork session without a clear hypothesis, we rely on luck. Conversely, when we utilize structured testing, we rely on anatomy. It is insufficient to know where a muscle attaches; you must understand how it functions within a kinetic chain. If a runner complains of knee pain, a relaxation therapist treats the knee. A sports medicine therapist, however, examines the hip and ankle. This depth requires conducting thorough assessments to identify asymmetries and compensations, guiding us away from referred sensations and toward the actual lesion.
Foundations of Client Assessment
The intake process establishes the therapeutic relationship. Organization is key here; a chaotic intake leads to missed red flags. We begin with a detailed medical history to understand the client condition, including past surgeries and daily repetitive motions. Assessment ethics dictate that we screen for contraindications immediately to ensure safety.
Subjective questioning helps us map the nature of the complaint. Sharp, electrical sensations suggest nerve involvement, while dull aches point toward muscular issues. This verbal evidence directs our physical investigation.
Visual and Palpation Assessment Protocols
Once we have the history, we move to observation. This is divided into static and dynamic analysis.
Static and Gait Analysis
We observe the individual standing, checking for deviations from anatomical neutral, such as the height of the iliac crests or forward head posture. However, static posture tells only half the story. A gait assessment reveals how the body manages load during movement. I advise students to watch the client walk before the formal session begins.
We look for specific phases of the gait cycle. Does the foot land neutrally at heel strike? Is there sufficient extension at the big toe? A lack of hip extension during walking often forces the lumbar spine to extend instead. By identifying this pattern, we know to treat the hip flexors rather than just the lower back.
Palpation Assessment
After visual inspection, we use touch to verify our findings. Palpation assessment allows us to read the state of the tissue. We are assessing temperature, texture, and tone.
Skilled palpation requires “listening hands.” If you press too hard, the body guards against you. You must sink in slowly to detect subtle differences in muscle tension. Healthy muscle should be resilient; boggy tissue suggests congestion, while stringy texture suggests chronic ischemia.
Orthopedic Testing and the Adson Test
To pinpoint specific pathologies, we employ orthopedic tests. Musculoskeletal conditions often mimic one another. For instance, pain radiating down the arm could be a cervical disc herniation or Thoracic Outlet Syndrome (TOS). To differentiate, we utilize the Adson Test.
Performing the Adson Test
This test evaluates the anterior scalene muscle and its potential compression of the neurovascular bundle.
- The individual sits upright.
- The therapist locates the radial pulse on the affected arm.
- The arm is extended, abducted, and externally rotated.
- The individual takes a deep breath, holds it, and rotates their head toward the affected side.
If the radial pulse diminishes or disappears, or if symptoms are reproduced, the test is positive. This indicates the scalenes are compressing the artery or nerves. Consequently, the treatment plan must focus on releasing the scalenes and mobilizing the first rib, rather than treating the hand where the symptoms are felt. We use these tests to identify common injuries and differentiate between muscle strain and ligament sprain.
Trigger Point Mechanics and the Bodywork Session
A major component of remedial massage is the identification of trigger points. A trigger point is a hyperirritable spot within a taut band of skeletal muscle that produces referred pain.
Understanding these patterns is crucial. A trigger point in the upper trapezius often refers pain into the temple, mimicking a headache. The client may request a head massage, but the source is the shoulder. We use ischemic compression to address these points, distinguishing between active points that cause current pain and latent points that are only painful upon pressure.
Integrating these findings turns a routine massage into effective therapy. If we find limited hip extension, we might employ muscle-resistance techniques, such as Proprioceptive Neuromuscular Facilitation (PNF), to reset the muscle’s resting tone.
The Future of Massage Therapy
The field of massage therapy is evolving toward a neuro-physiological approach. Practitioners who refuse to update their assessment skills will be left behind.
At RSM, we view injuries as puzzles. By applying rigorous assessment methods, we honor the complexity of the human body. We do not just rub where it hurts; we determine why it hurts.
We must remember that the body functions as a unit. A holistic approach recognizes that physical tension often correlates with psychological stress. Our manual techniques address the tissue, but we may also need to coach clients on breathing to facilitate true healing.
The Blueprint for Clinical Mastery
Effective treatment is impossible without accurate assessment. Whether you are checking a radial pulse or analyzing a gait cycle, every piece of data matters. If you are serious about your career, commit to mastering these methods. Your hands are your tools, but your assessment skills are the blueprint. Without the blueprint, you cannot build a lasting structure of health.
Integrating Orthopedic Massage with Other Modalities in Practice
Orthopedic Massage Course Chiang Mai
Musculoskeletal rehabilitation is rarely a linear process. In my years practicing sports medicine, I have observed that the most successful recovery outcomes occur when practitioners refuse to work in isolation. A single pair of hands can achieve remarkable results; however, the human body is a complex system of levers and chemical signals that often requires a multi-disciplinary approach. In RSM’s Orthopedic Massage Course, we emphasize that manual therapy is a critical component of a larger ecosystem.
When a client presents with chronic dysfunction, it is rarely just a tissue problem. It is a functional problem. Orthopedic massage focuses on restoring soft tissue balance, but without addressing movement patterns or joint mechanics, the dysfunction often returns. This leads to the necessity of collaboration. By viewing the body through a wider lens, we can see where manual techniques intersect with physical therapy, strength conditioning, and other clinical interventions.
Defining Orthopedic Massage in Clinical Settings
Orthopedic massage is distinct from general relaxation techniques. It is a systematic approach to treating musculoskeletal issues through assessment and manipulation. We do not guess where the problem lies; we assess. Once the pathology is identified, specific massage techniques are applied to structures to reduce tension and improve circulation.
The efficacy of this method increases significantly when it is part of a broader healthcare plan. For instance, a patient recovering from surgery requires precise loading protocols. However, the surrounding musculature often enters a protective spasm. Orthopedic massage is often integrated here to normalize muscle tone. Consequently, the patient can perform their rehabilitation exercises with greater accuracy.
Collaboration with Physical Therapy
The relationship between manual therapists and physical therapists should be symbiotic. Physical therapy primarily addresses movement dysfunction, strength deficits, and neurological control. In contrast, our work addresses the quality of the tissue that executes those movements.
When a muscle is hypertonic, it cannot contract efficiently. This results in poor biomechanics. If a physical therapist prescribes a squat pattern to strengthen the glutes, but the hip flexors are rigid, the patient will compensate. Integration of manual therapy at this stage changes the equation. By releasing the hip flexors first, we create a window of opportunity where the patient gains an increased range of motion. Specifically, they can now access the correct muscle groups during their PT session.
We teach our students to communicate effectively with other healthcare providers. You must speak the language of anatomy. When you can articulate that your treatment plan aims to reduce inhibition to facilitate better movement, you become a valued partner in the rehabilitation team.
Why Massage Complements Chiropractic Care
Chiropractic care focuses heavily on the alignment and mobility of the joint. The skeletal system relies on the muscular system for stability. If a chiropractor adjusts a vertebral segment but the surrounding paraspinal muscles remain in a state of chronic spasm, the adjustment seldom holds.
Conversely, if massage is applied before the adjustment, the tissue becomes pliable. The resistance drops. This allows the chiropractor to perform the manipulation with less force. Alternatively, performing massage post-adjustment can help the nervous system integrate the new structural position.
I have frequently worked alongside chiropractors to manage complex spinal cases. The synergy is undeniable. Chiropractic addresses the hard tissue; we address the soft tissue. Together, we break the pain-spasm-pain cycle. This leads to longer-lasting relief for the patient.
Integrating Orthopedic Massage with Deep Tissue Work
There is often confusion regarding the difference between deep tissue work and orthopedic protocols. While they share similarities, our approach is assessment-driven. However, deep tissue modalities are valid tools within the orthopedic framework.
Deep pressure is effective for accessing lower layers of fascia. Management of chronic pain often requires reaching these depths to stimulate a mechanoreceptor response. When we apply deep, slow pressure, we lower the sympathetic nervous system’s “fight or flight” response. As a result, the patient’s pain threshold modulates.
Using deep tissue requires skill. It is not about force; it is about sinking into the tissue. If you force the tissue, it fights back. If you sink, it yields. Combining specific assessment with the broad strokes of deep work provides a comprehensive reset for the neuromuscular system.
Addressing Therapy for Pain and Trigger Points
Pain is a subjective experience driven by nociceptive signals. Treating musculoskeletal issues effectively requires understanding that pain is not always located at the source of the problem.
A specific component of our work involves the trigger point. This hyper-irritable spot in the skeletal muscle is associated with a hypersensitive nodule. Trigger point techniques are highly compatible with our protocols. When a patient has referral pain, identifying the active trigger point is often the key to resolution. However, simply pressing on a spot is rarely enough. We must prepare the tissue around it.
Effective therapy involves deactivating the point and then lengthening the muscle to prevent reactivation. If we ignore the trigger point, the muscle remains short. If we ignore the surrounding fascia, the trigger point returns. Consequently, a blended approach yields the best results.
Combining Massage with Strength Training
Sports massage is a modality specifically designed for the athletic population. Integrating this with strength and conditioning is vital for the modern athlete.
High-volume training creates micro-trauma in the muscle fibers. This is necessary for growth, but it also produces metabolic waste. Sports massage accelerates the flushing of these byproducts. However, timing is critical. Deep, aggressive work immediately before a heavy lift can reduce muscle tonus too much, potentially destabilizing the joint.
Conversely, post-training massage aids in shifting the body from a sympathetic state to a parasympathetic state. This shift is where recovery happens. We provide heavy work on rest days and lighter, activation work on game days to align with the athlete’s schedule.
Future Trends in Other Therapies
The field of sports medicine is evolving. We are seeing a rise in other therapies being combined with manual work. Instrument Assisted Soft Tissue Mobilization (IASTM), cupping, and dry needling are becoming commonplace.
While these tools are valuable, they do not replace the skilled human hand. Tools provide a different sensory input. Our protocols serve as the foundation, while these modalities act as specialized adjuncts. Integration forces us to remain humble students. I constantly research new findings in fascial science to refine our curriculum at RSM.
An Integrated Approach for Clients
The ultimate goal of any treatment is patient autonomy. We want our clients to return to their lives without dependency on us. Education is part of this process. When we combine manual treatment with education about posture and self-care, we empower them.
An integrated model often looks like this:
- Assessment identifies the dysfunction.
- Manual work restores tissue quality and reduces acute symptoms.
- Corrective exercise reinforces the new range of motion.
- Lifestyle modification prevents recurrence.
When clients understand that their massage is part of a logical progression, compliance improves. This leads to sustainable results. At RSM, we emphasize that you are not just a person who rubs muscles; you are a educator and a clinician.
The era of the isolated practitioner is fading. As our understanding of the human body deepens, the lines between modalities blur. This is a positive development. It means we are focusing less on protecting our specific professional turf and more on solving the patient’s problem.
Orthopedic massage provides a unique contribution to this mix. It offers the tactile feedback that machines cannot replicate. But it shines brightest when it is part of a team effort. I encourage all my students to look outward. Build relationships with chiropractors and physical therapists. Learn how your massage fits into their protocols. By embracing this mindset, we elevate the entire profession of sports medicine and move closer to the ideal of holistic recovery.
How to Identify Fascial Restrictions: A Technical Guide to Pain and Fascia

Clinical Palpation Training for myofascial restriction
The Hidden Architecture of Movement
The human body is an interconnected architecture where no single part functions in isolation. In RSM’s Myofascial Release Course, we teach that effective sports medicine requires looking beyond localized symptoms. Often, the root cause of chronic issues lies within the connective tissue network known as fascia.
Fascia is a continuous web surrounding every muscle, bone, and organ. When healthy, this tissue glides effortlessly, allowing fluid movement. However, trauma or repetitive strain can alter its physical properties, causing densification. This leads to fascial restrictions that compromise the entire biomechanical system. A restriction in the foot can easily transmit tension upward, manifesting as pain in the lower back. Therefore, to effectively treat the patient, we must treat the web, not just the isolated part.
Understanding Fascia and Movement Mechanics
To detect dysfunction, one must understand how healthy tissue behaves. Healthy connective tissue is thixotropic; it becomes fluid when warmed and moved. When areas of the body lose this adaptability, the mechanics change, and the body compensates to avoid pain.
If fascial tightness occurs in the anterior hip, the lumbar spine often hyperextends. This creates secondary pain patterns that distract inexperienced therapists. We analyze movement to spot these compensations. A restriction acts like a snag in a sweater – the pull is felt everywhere, but the knot is in one specific spot. Static palpation alone is insufficient because it fails to reveal where the “fabric” fails to glide.
Diagnosing Fascial Tightness and Tissue Texture
Manual assessment is the most reliable tool for diagnosing fascial issues. Unlike standard muscle palpation, which presses perpendicular to the fiber, assessing connective tissue requires shearing or gliding motions.
I teach students to use “skin rolling” to find these adhesions. This involves lifting a fold of skin and rolling it. In healthy areas, this fold moves like a wave. In areas of tightness, the skin adheres to the underlying layers, feeling thick and unyielding. Another method is the “fascial glide,” where you slide superficial tissues over deeper structures. A restriction presents as a hard barrier, preventing the hand from sliding in a specific direction. This points us directly toward the source of the tension.
Recognizing Pain and Myofascial Restriction
Pain signals in fascia differ significantly from muscular strain. Muscle injuries usually cause sharp, localized discomfort. In contrast, fascial pain is often described as a deep, burning ache or a squeezing sensation. It can be diffuse, making it difficult for the patient to pinpoint.
This type of discomfort typically worsens with inactivity. Patients report feeling stiff upon waking, as the lack of movement causes the fascial fluids to become viscous. Trigger points are another hallmark of myofascial restriction. While located within the muscle, their persistence is often linked to the surrounding fascial environment. Compressing these points reproduces familiar pain, confirming fascial involvement.
Distinguishing Muscle Issues from Fascial Involvement
Differentiating between a tight muscle and a restricted fascial sheet requires a refined touch. A tight muscle often relaxes via reciprocal inhibition when the opposing group contracts. Fascial tissue does not. It relies on plastic deformation rather than neurological relaxation.
When you stretch a muscle, it has an elastic recoil. Conversely, restricted fascia feels leathery and hits an abrupt stop. We also look for “silenced” muscles. If a fascial compartment becomes too tight, it increases internal pressure and inhibits the muscle’s ability to contract. If a patient tests weak without nerve damage, I immediately investigate the surrounding fascia for restrictions.
Palpation Techniques to Locate Areas of Restriction
Developing a “listening hand” is essential. When engaging a barrier, you must meet the resistance without forcing through it. We use fingertips to trace the septa between muscles, as these dividing walls are common sites for adhesions.
For broader sheets, such as the thoracolumbar fascia, we use the flat of the forearm to assess tone. We look for areas that feel cooler or appear paler, which indicates reduced blood flow caused by chronic tension. We combine this with functional tests. By loading specific myofascial lines – such as dorsiflexing the ankle during a hamstring stretch – we can determine if the limitation is muscular or if it is restricting movement through the entire chain.
The Role of Therapy in Treating Restrictions
Once we identify these barriers, the goal of therapy is to restore the glide potential. We do not force the tissue; force causes inflammation. Instead, effective treatment uses slow, sustained shearing forces. This input generates heat, lowering the viscosity of the fluids between layers and allowing them to release.
This process is known as “creep.” Viscoelastic tissue deforms slowly under constant load. Successful release is marked by a palpable softening, increased local blood flow (redness), and an immediate drop in pain levels.
Precision in Manual Medicine
Identifying fascial restrictions is an art grounded in science. At RSM, we emphasize that you cannot treat what you cannot feel. By systematically assessing skin mobility and tissue texture, we find the exact location of the blockage. This allows us to correct the architecture rather than just chasing symptoms. When the fascia is free, movement becomes fluid, and the body returns to optimal function.
Developing Effective Pressure Techniques in Massage for Clinical Results

Hironori is invited to the 5 star wellness resort spa for massage training
Force is the primary language of manual therapy. It serves as the medium through which a therapist communicates with the nervous system and the musculoskeletal architecture. At RSM International Academy, we often observe students confusing force with effort. They believe that resolving chronic restriction requires physical exertion. This misconception leads to therapist burnout and defensive guarding in the client. I designed our Deep Tissue Massage Course curriculum in Chiang Mai to correct this fundamental error. True clinical efficacy comes from precision, not power.
Understanding the physics of force application allows a therapist to bypass the body’s natural defense mechanisms. When we apply force correctly, we engage the parasympathetic nervous system. This allows the tissue to melt rather than resist. Conversely, aggressive or poorly calibrated force triggers a sympathetic response. The muscle tightens to protect itself. This negates the therapeutic intent.
The Science of Pressure in Massage Therapy
We must first define what happens beneath the skin. Pressure is a mechanical stimulus that creates a biological response known as mechanotransduction. The cells perceive physical deformation and convert it into biochemical signals.
The skin and fascia are densely populated with mechanoreceptors. Ruffini endings, for instance, detect sustained pressure and stretching. When a massage therapist applies a slow, sinking force, they communicate with these receptors to lower the tonus of local motor units. However, if the application is too sharp, nociceptors activate. This triggers a withdrawal reflex, causing the muscle to contract. We teach students to visualize sinking through layers of water; you cannot force your way to the bottom without creating turbulence. You must wait for the tissue to accommodate the intrusion.
Differentiating Deep Pressure from Deep Tissue
Terminology in this field is often imprecise. Clients frequently request “deep tissue” when they actually want “heavy pressure.” As sports medicine professionals, we must distinguish between the two. Deep tissue massage refers to a specific modality targeting the sub-layer of musculature. It requires a slow pace and minimal lubrication to engage the tissue without sliding.
Deep pressure, in contrast, is simply a subjective sensation of intensity. One can apply deep pressure to superficial muscles or light pressure to deep muscles. The confusion arises because clients associate pain with effectiveness. They believe that if it does not hurt, it is not working.
This is a dangerous fallacy. Excessive force causes micro-trauma, inflammation, and rebound tenderness. We educate our clients that the most effective massage occurs at the “functional edge.” This is the threshold where the client feels a satisfying intensity but can still breathe normally. If the client holds their breath or clenches, the nervous system has shifted into defense mode.
Biomechanics and Sustainable Techniques
The longevity of a therapist’s career depends entirely on their body mechanics. The high attrition rate in massage is largely due to joint failure in the thumbs and wrists. Therapists who rely on muscular effort to generate pressure will inevitably injure themselves.
Effective techniques rely on stacking the joints. When the shoulder, elbow, and wrist align, the skeletal structure transmits the force. The muscles of the arm remain relaxed. This allows the therapist to use their body weight rather than their triceps. I constantly remind students that body weight is a free resource. Gravity does not get tired; muscular effort does.
Power originates from the ground. A therapist generates force by leaning from the ankles and hips using lunge mechanics. The back leg provides the drive while the front leg provides stability. By shifting the center of gravity forward, the therapist increases pressure. This creates a fluid application that is comfortable for the client and sustainable for the therapist.
The Mechanics of Trigger Point Therapy
A significant portion of pain complaints stems from myofascial trigger points. These are hyperirritable spots within a taut band of skeletal muscle. A trigger point consists of sarcomeres stuck in a contracted state, compressing local capillaries and restricting blood flow. This metabolic crisis sensitizes nociceptors, causing pain.
Point therapy aims to resolve this issue through ischemic compression. The therapist applies sustained pressure directly to the nodule. This mechanically forces blood out, inducing temporary ischemia. Upon release, fresh, oxygenated blood rushes in to flush out inflammatory metabolites.
Treating a trigger requires extreme sensitivity. If the pressure is too light, it fails to release the contraction. If it is too heavy, the pain causes a reflex contraction. We use a pain scale of 1 to 10, aiming for a 7. At this level, the client experiences discomfort that feels productive. As the trigger point releases, the sensation of pain should diminish even if the force remains constant.
Assessing Muscle Tension and Safety
Before applying force, a therapist must assess the landscape. Palpation is the art of seeing with the fingers. Muscle tension manifests differently depending on its cause. Protective guarding feels hard and rubbery. Intrinsic spasm feels like a distinct knot. Fibrosis feels leathery.
Each condition requires a different approach. Guarding requires soothing compression to calm the nervous system. Fibrosis requires friction to break down adhesions. The most skilled therapists practice active listening with their hands. As you sink into a muscle, you feel a barrier. An amateur pushes through it; a master waits at the barrier. By holding steady, you invite the tissue to yield through a phenomenon called creep.
Navigating Client Pressure Preferences
Perception of pressure is subjective. It is influenced by hydration, stress, and pain tolerance. Therefore, client pressure feedback is vital. However, verbal feedback has limitations. Clients often say “pressure is fine” to avoid offending the therapist.
I teach students to rely on non-verbal cues. Flinching, shallow breathing, or curling toes are signs that the pressure is excessive. Conversely, if a client is not responding, the pressure may be insufficient. We must constantly adjust. The body is not a static object; it is a reactive biological system.
Clinical Safety and Contraindications
High-pressure techniques carry risks. It is imperative to understand anatomy to avoid injuring the client. Endangerment sites like the popliteal fossa, axilla, and anterior neck contain unprotected neurovascular bundles. Compressing these areas can cause damage. Furthermore, applying deep pressure to clients with osteoporosis or active inflammation is contraindicated. A comprehensive intake and assessment must precede any hands-on massage therapy.
Integrating Science into the Art of Touch
The development of pressure skills is a lifelong pursuit. It requires a knowledge of physics to apply force efficiently, anatomy to apply force safely, and neurology to apply force therapeutically.
At RSM International Academy, we do not view massage as merely relaxation. We view it as a clinical intervention. The difference between a mediocre treatment and a medical intervention lies in the quality of the pressure. Is it intelligent? Is it responsive? Is it anatomically precise?
When a therapist masters this effective pressure technique, they stop struggling against the body. They begin to work with it. The client feels the difference immediately. They feel safe, and they feel the tissue change. This is the standard of excellence we strive for. It elevates the profession and delivers the results that clients in pain are desperately seeking.
Postural Assessment: The Role of Postural Analysis in Remedial Massage

Deep Tissue Massage for lower cross syndrome
Effective treatment in sports medicine rarely begins on the table. It begins the moment a client walks through the door. At RSM International Academy, and in our Remedial Massage Course, we operate on the philosophy that pain is often a symptom of a broader structural issue rather than an isolated event. Treating the site of pain without understanding the architectural context of the body often leads to temporary relief rather than long-term resolution.
For massage therapists aiming to work at a clinical level, the ability to read the body before applying touch is non-negotiable. We must move beyond simple relaxation techniques and engage with the anatomical reality of how a person stands, moves, and bears weight against gravity.
The Science of Postural Analysis
The human body functions as a tensegrity structure, relying on a balance of compression and tension. When this balance is compromised, the body compensates. A practitioner who understands these mechanics can trace a client’s chronic lower back pain to a collapsed arch in the foot or a rotated pelvis. This investigative process is the core of our sports medicine curriculum in Chiang Mai.
Postural analysis serves as a roadmap for the treatment plan. It allows us to distinguish between the source of the pain and the site of the pain. Postural stability is key to long-term health; therefore, our goal is to restore equilibrium. If a client presents with tension headaches, working solely on the neck treats the effect. The cause is often a structural imbalance in the thoracic spine or shoulder girdle.
Performing Effective Posture Assessments
A systematic approach ensures consistency. The screening process typically involves observing the client in a standing position against a plumb line. This provides a vertical reference point to measure deviations.
The practitioner observes symmetry from the anterior view. We look for whether the head tilts or if the shoulders are level. Even a minor discrepancy can indicate a pelvic torsion. This visual data reveals valuable information about how the client loads their joints. Conversely, the lateral view offers insight into spinal curvature. Here, the spine assessed against gravity tells a story of compensation, such as hyper-kyphosis. These distortions influence muscle tone, creating areas that are locked short or locked long.
Identifying Postural Imbalance
Static observation provides a baseline, yet the body is designed for motion. A static postural evaluation must be complemented by assessing movement patterns. A client may appear symmetrical while standing still but exhibit significant dysfunction during a gait test.
Postural imbalance often manifests during these dynamic tests. For instance, valgus stress at the knee during a squat indicates weakness in the gluteus medius. This leads to specific tension patterns that the therapist must address. Remedial massage is most effective when it targets the specific tissues reinforcing these habits.
The client’s posture is a habit formed over years. It is shaped by occupation and sports activities. Recognizing these patterns allows us to tailor the therapy session to lengthen shortened structures and stimulate weak ones.
What the Patient Reveals
Bones do not move themselves; muscles move bones. Therefore, every skeletal deviation has a corresponding soft tissue correlate. When we identify imbalances in the skeleton, we simultaneously identify the state of the myofascial system.
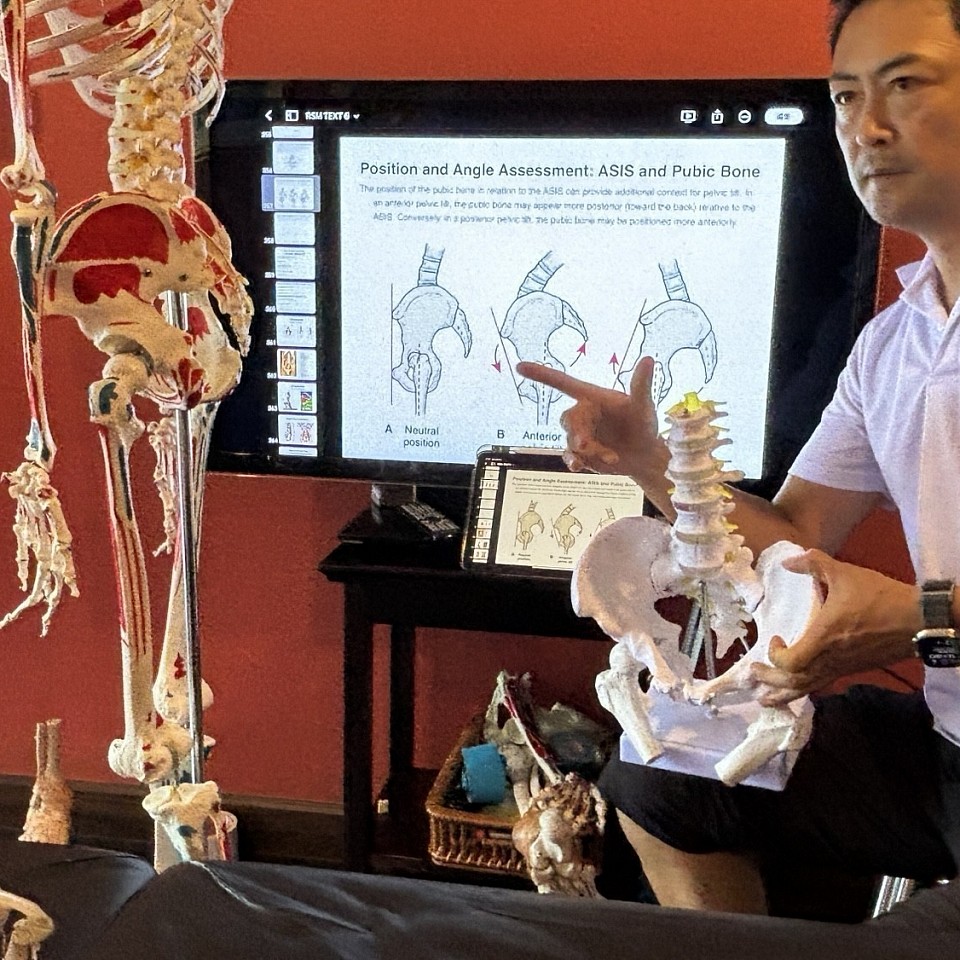
A postural assessment helps us predict trigger point locations. An anterior pelvic tilt almost guarantees tight hip flexors and lumbar erectors. This diagnostic capability elevates massage therapy from a luxury to a necessary component of healthcare. It builds trust. When you can articulate to a patient why they feel pain based on their stance, you demonstrate clinical competence.
Integrating Assessments into Therapy
The transition from assessment to treatment must be seamless. The data collected dictates the protocol. If the body mechanics suggest an Upper Crossed Syndrome, the session focuses on releasing the pectorals. The postural massage strategy must adapt as the body changes. We recommend re-evaluating the body posture periodically to track progress.
Below is a brief overview of common indicators:
- Head Forward Posture: Indicates strain on posterior cervical muscles.
- Internal Shoulder Rotation: Suggests tight pectorals and latissimus dorsi.
- Anterior Pelvic Tilt: Associated with tight hip flexors.
- Foot Pronation: Causes internal rotation of the tibia.
There is a distinct difference between spa treatments and remedial services. The latter requires an analytical mind. By integrating a thorough evaluation, we ensure that our work creates lasting change. Postural analysis is not just about finding what is wrong; it is about understanding how the body survives, and helping it function more efficiently.
The Science of Myofascial Release for Improving Posture

Dynamic Myofascial Release for upper cross syndrome
Structural integrity relies on more than just skeletal stacking. Fascia, the continuous connective tissue network enveloping every muscle and organ, dictates the resting position of our anatomy. During RSM International Academy's Myofascial Release Course, I teach that fascia is not merely passive wrapping; it is a sensory organ capable of contraction and profound rigidity. When this network becomes distorted, the skeletal structure follows.
Correcting these deviations requires more than a conscious effort to “stand up straight.” Volitional control cannot override the tensile strength of thickened connective tissue. This is why manual therapy is essential. Myofascial release offers a mechanical advantage by addressing the collagenous matrix holding the body in misalignment.
Understanding the Mechanics of Myofascial Release
Myofascial release is a specialized manual therapy designed to sustain pressure into restrictions to eliminate pain and restore motion. To understand its efficacy, we must look at tissue composition. Fascia consists of elastin, collagen, and a gel-like ground substance. In a healthy state, this system is fluid.
However, trauma or repetitive static positioning causes the ground substance to solidify, changing from a fluid sol state to a gel state. Collagen fibers cross-link, thickening the tissue and shortening the muscle length. We define this as a restriction.
When a therapist applies sustained pressure, they engage the piezoelectric effect. This mechanical pressure generates a low-level electrical charge, signaling fibroblasts to reorganize the collagen matrix. Simultaneously, heat and friction liquefy the ground substance. As a result, the fascial layers regain their ability to glide. Unlike Swedish massage, which uses rhythmic strokes, release techniques require a slow, sinking engagement to penetrate the deeper layers where postural patterns reside.
How Bad Posture Develops in the Tissue
The body operates on tensegrity, where bones act as compression struts floating in a sea of fascial tension. When specific fascial lines shorten, they pull the skeleton out of alignment. Consider the “Anterior Superficial Line.” If an office worker spends hours hunched over, the fascia in the chest and abdomen shortens.
This creates a permanent downward pull. Even when standing, this tight fascia drags the shoulders forward. The posterior muscles are then forced to remain in a stretched, weakened state to keep the head upright. This leads to bad posture and chronic fatigue. Treating the back pain directly often fails because the pain is merely a symptom of the antagonist muscles losing the battle against anterior tension. At RSM, we hunt for the restriction, not just the pain. By lengthening the anterior structures, we remove the drag, allowing the shoulders to drift back into a neutral position.
Addressing Neck Tension and Alignment
Forward Head Posture (FHP) is a pervasive issue in modern society. For every inch the head migrates forward, the load on the cervical spine increases, placing immense strain on the neck. Fascial restrictions in the suboccipital region function like a clamp at the base of the skull, impinging nerves and reducing range of motion.
Correcting this requires engaging the tissue barrier and waiting for a neurological response. The fascial network is rich in mechanoreceptors. Slow, sustained pressure stimulates these receptors to inhibit sympathetic nervous system activity. This lowers global muscle tonus, allowing the neck to relax.
We also observe that tension in the jaw travels down the anterior neck, pulling the head forward. Release work on the masseter and temporalis muscles often contributes to immediate improvements in cervical positioning.
Self-Myofascial Release for Daily Maintenance
While professional treatment is vital, gravity acts on the body constantly. Therefore, patients need a daily counter-measure. Self-myofascial release (SMR) empowers individuals to manage their own tissue health using tools to mimic a therapist’s hands.
The most common tool is the foam roller. However, the application must be precise. Rapidly rolling back and forth does little to change tissue density. To achieve a true release, the user must locate the point of highest tension and pause.
Effective SMR Protocols:
- Quadriceps: Lying prone with the foam roller under the thighs releases the superficial front line, which is crucial for correcting anterior pelvic tilt.
- Thoracic Spine: Lying supine with the roller across the shoulder blades helps reverse the kyphotic curve of the upper back.
- Latissimus Dorsi: Rolling the side of the rib cage opens the pathway for the arms to hang naturally.
We also recommend using firmer tools, like lacrosse balls, for detailed work in the glutes. These smaller points of contact penetrate deeper than a broad cylinder can.
Long-Term Release and Structural Health
Correcting poor posture is a process of re-education. Once the restriction is removed, the muscles must be strengthened in their new, optimal range. If a patient receives a treatment but returns to poor habits, the fascia will stiffen again.
We advocate a three-pronged approach:
- Release: Manual therapy and self-myofascial work to unlock restrictions.
- Re-align: Conscious proprioception exercises to find a neutral spine.
- Reinforce: Strengthening the posterior chain to hold the new position.
Health is holistic. We cannot separate mechanical tension from the emotional burden it carries. Improving posture often correlates with improved confidence and respiratory function. Through the intelligent application of myofascial release techniques and a deep understanding of anatomy, we can reverse years of accumulation and restore the body to its natural design.
Addressing Specific Muscle Groups in Massage

Deep Tissue Massage and postural assessment
Understanding Anatomy and Physiology
At RSM International Academy, we believe that effective therapy begins with a profound understanding of the human body. A therapist cannot simply apply pressure blindly. Instead, they must visualize the structures beneath the skin. Knowledge of anatomy and physiology forms the foundation of our Deep Tissue Massage Course curriculum in Chiang Mai. This scientific approach ensures that every stroke serves a clear clinical purpose rather than just providing temporary relaxation.
Muscles are not isolated entities. They function within complex kinetic chains. When a student learns to identify how muscle groups are connected, they begin to see the body as an integrated system. Tightness in the hamstrings might cause pain in the lower back. Consequently, treating the site of pain without investigating the source often leads to temporary relief at best. We teach our students to look beyond the symptoms. They learn to map the origins and insertions of particular muscle groups to understand the mechanical failures causing the issue.
The body is layered. Superficial muscles cover deeper structures that are often the root cause of chronic dysfunction. Reaching these layers requires more than just physical strength. It requires an understanding of angles and tissue resistance. A highly effective way to treat these underlying issues is by visualizing the depth and direction of the muscle fibers. This visualization allows therapists to apply force that melts into the tissue rather than fighting against it.
Targeting Specific Muscle Groups for Rehabilitation
Precision is the hallmark of sports medicine. General full-body treatments have their place, but targeted massage offers superior results for rehabilitation. When we focus on relieving tension in a specific area, we can apply specialized techniques that would be impractical to use over the entire body.
For instance, an athlete suffering from rotator cuff issues requires a focused strategy. We isolate the supraspinatus or infraspinatus. This level of specificity allows us to address micro-traumas and scar tissue. Focusing on a single area allows the nervous system to process the changes being made to the soft tissue.
However, specificity does not mean ignoring the surrounding areas. We often find that muscle spasms in one area are a protective mechanism for a weakness elsewhere. Address particular muscles that stabilize the joint is just as critical as treating the prime movers. This comprehensive yet targeted approach is what differentiates a clinical sports massage from a spa treatment.
Effective Massage Treatment for Neck Muscles
The cervical region presents unique challenges due to its complexity and the density of sensitive structures. Neck muscles are prone to extreme tension due to modern posture habits. Treating this area requires a delicate balance of precision and pressure.
Many clients present with stiffness that radiates down into the shoulders. This often involves the levator scapulae and the upper trapezius. However, the deeper suboccipital muscles are frequently the culprits behind tension headaches. We train our students to palpate these small, dense muscles with care.
A massage session focused on the neck must respect the nerve pathways exiting the spine. Excessive force here can cause radiating pain or numbness. Conversely, pressure that is too light will fail to affect the dense fascia. Deep tissue massage in this region is effective but must be applied slowly. The therapist waits for the tissue to relax before sinking deeper. This patience prevents the muscles from seizing up in defense.
Trigger point therapy is particularly useful here. Identifying hyper-irritable spots within the sternocleidomastoid or scalenes can resolve referred pain patterns that mimic migraines. By applying sustained compression, we encourage the muscle to release its holding pattern. This restores blood flow and reduces the chronic neural noise contributing to the client’s discomfort.
Trigger Point Protocols and Deep Massage
Pain often manifests as localized knots or adhesions. Friction is a technique we utilize to break down these cross-fiber adhesions. Friction massage involves applying pressure across the grain of the muscle fiber. This action helps realign collagen fibers during the remodeling phase of injury recovery.
We frequently combine friction with deep tissue protocols. Deep tissue massage is not synonymous with “hard” massage. It refers to targeting the sub-layer of musculature and fascia. To reach the deep layers, the therapist must sink through the superficial layers without triggering a guarding response. This requires slow, melting pressure.
When muscle fibers are stuck together, they cannot glide properly. This friction reduces range of motion and causes inflammation. Tissue massage aimed at separating these fibers restores mobility. We see this often in the IT band or the paraspinal muscles. By clearing these restrictions, we boost muscle recovery significantly.
However, deep work can cause soreness. It is vital to communicate with the client. We explain that pain during treatment should be “good pain” – a sensation of release rather than sharp, neural feedback. If the body tenses up, the pressure is too aggressive. The goal is to coax the tissue into relaxation, not to force it.
The Role of Sports Massage in Injury Prevention
Sports massage serves a dual purpose: recovery and prevention. By maintaining the elasticity of the soft tissue, we reduce the risk of strains and tears. An injury often occurs when a muscle is too tight to absorb the shock of a sudden movement. Regular, focused work keeps the tissues compliant.
We emphasize that massage therapy is a crucial component of an athlete’s training regimen. It is not a luxury. It is maintenance. Just as a mechanic tunes an engine, a sports massage therapist tunes the musculoskeletal system.
In our academy, we simulate real-world scenarios. Students practice identifying imbalances before they become injuries. They learn to feel the difference between hypertonic tissue and healthy tone. This tactile intelligence is what allows them to deliver high-quality care.
Neuromuscular massage techniques also play a role here. By communicating with the nervous system, we can reset the resting tone of a muscle. This is often more effective than mechanical pressure alone. It retrains the brain-muscle connection, leading to longer-lasting results.
Practical Application for the Back and Spine
The back is the most common area of complaint. It houses the spine, which is the central highway for the nervous system. Treatment here must be systematic. We do not simply rub the back. We assess the erector spinae, the quadratus lumborum, and the multifidus.
Chronic lower back pain often stems from imbalances in the pelvis. Therefore, effective treatment of the back often involves work on the glutes and hamstrings. We utilize deep tissue techniques to lengthen short hip flexors that might be pulling the lumbar spine into lordosis.
For thoracic issues, we look at the rhomboids and the interplay with the pectorals. A hunched posture stretches the back muscles and shortens the chest muscles. Treating only the back provides relief, but treating both sides addresses the posture. This holistic view of specific segmentation within a global context is key.
Our goal is to produce therapists who are critical thinkers. They do not follow a script. They analyze the tissue under their hands and adapt their strategy in real-time. Whether it is resolving spasms in the lumbar region or mobilizing the thoracic cage, the focus remains on anatomical precision.
- Assessment: Check range of motion and identify pain patterns.
- Warm-up: Increase blood flow to the area.
- Specific Work: Apply deep techniques and friction to adhesions.
- Integration: Connect the treated area back to the rest of the body.
This structured approach ensures safety and efficacy. It transforms a standard massage into a sports medicine intervention. By respecting the anatomy and applying focused force, we facilitate true healing.
Myofascial Release vs Traditional Stretching: Understanding the Physiological Differences
Posture Assessment and Myofascial Release
In our Myofascial Release Course at RSM International Academy, we emphasize that soft tissue restriction is not a static definition, but a dynamic variable. One of the most frequent corrections I make during practical training involves students attempting to address limited range of motion by solely focusing on stretching. They see a shortened muscle and instinctively try to pull it into length. However, this approach often overlooks the complex architecture of the fascial system. To truly master rehabilitation, a therapist must visualize the difference between elongating a muscle fiber and releasing the fascial matrix that encases it.
There is a distinct clinical difference between elongating a muscle via tensile force and reorganizing connective tissue through direct manipulation. While both aim to improve health, they operate through fundamentally different physiological mechanisms. Understanding these differences allows practitioners to build more effective treatment plans for physical rehabilitation.
The Mechanics of Myofascial Release
Many practitioners conflate general massage with specific myofascial release. While they may look similar, the intention and tissue response are distinct. Myofascial release targets the deep fascia and intramuscular septa rather than the muscle belly alone.
Fascia is a non-Newtonian fluid matrix with thixotropic properties—it becomes fluid when agitated by heat and pressure, and solid (gel-like) when sedentary. When we apply the sustained shearing pressure characteristic of MFR, we do not force the tissue apart. Instead, we stimulate a phase change in the ground substance, allowing collagen layers to glide.
Traditional approaches often miss this nuance. If fascial layers are densified due to inflammation, simply pulling the limb will not separate them. The tissue requires a specific shearing force to restore the sliding mechanism before length can be achieved.
Why Traditional Stretching Often Hits a Plateau
While stretching is vital for fitness, relying on it as the sole method for correcting dysfunction has limitations. Static stretching primarily targets the viscoelastic properties of the muscle-tendon unit.
However, a mechanical barrier often prevents elongation. Imagine a rubber band with a knot tied in the center. If you pull both ends, the knot tightens rather than unravels. Similarly, when traditional stretching is applied to a muscle with adhesions, the healthy tissue stretches while the adhered segments lock down. This explains why many athletes stretch daily yet see no improvement in flexibility. The tension is a fascial architectural issue, not just a muscle length issue.
Comparative Effects on Tissue and Performance
To clarify the specific roles of these modalities, we must look at how they are compared regarding their effects on the body. At RSM, we teach students to differentiate these tools based on the specific pathology they are treating.
Here are the key myofascial stretching differences:
- Target Tissue: Traditional stretching targets sarcomeres. Myofascial release targets the parallel elastic component (fascia).
- Mechanism: Stretching exercises use tensile strain to induce creep. Release therapy uses shearing force to induce thixotropy.
- Neural Effect: Aggressive stretching can trigger the myotatic reflex (protective contraction). Release work down-regulates the gamma loop system to reduce tone.
Fascial Stretch Therapy and Pain Management
Chronic pain is rarely isolated to a single structure. It is often the result of cumulative load on the kinetic chain. When working with clients, we often find the site of pain is merely the victim, while the criminal is a restricted fascial line elsewhere.
In this context, fascial stretch therapy (FST) becomes highly effective—but only when the tissue quality allows for it. FST differs from standard static holds because it often involves traction and oscillation. However, even this advanced therapy requires pliable tissue.
If a client presents with a fibrotic fascial system, forcing range of motion can cause micro-tearing. The sequence of treatment is critical. We must first address the densification. Once the layers are hydrated, we can introduce fascial stretch techniques to re-educate the range of motion.
The Role of SMR and Integration
For clients to maintain results, we often prescribe self-care. SMR (Self-Myofascial Release) acts as daily “flossing” for the fascia. By compressing the tissue using foam rollers or balls, the client forces fresh fluid into the interstitial spaces.
However, students must understand the difference between SMR and stretching. Rolling rapidly creates heat but may not release deep restrictions. Slow, sustained pressure is required to engage the barrier.
We do not advocate abandoning stretching. Rather, we advocate for the correct sequencing of care. The most effective protocol for restoring physical capacity follows a specific order:
- Release: Use manual techniques or SMR to hydrate tissue.
- Mobilize: Perform active drills to engage neuromuscular control.
- Stretch: Apply fascial stretching or dynamic stretching to set the new length.
This is particularly vital for the spine. The thoracolumbar fascia acts as a force transmitter. Tightness here is rarely solved by flexion stretching, which can irritate lumbar discs. A myofascial stretching approach first releases the glutes and lats anchoring into this fascia. Once freed, the stretch becomes a tool for decompression rather than a battle against a barrier.
On Clinical Application
At RSM International Academy, our goal is to produce therapists who think critically. Recognizing the distinction between myofascial release and traditional elongation techniques allows for precision. We do not treat the body as a collection of parts, but as an integrated structure.
When a client asks about their limited mobility, the answer lies in the layers. Muscle cannot function optimally if it is encased in a rigid suit. By addressing the container (the fascia) before addressing the contents (the muscle), we unlock the body’s true potential for movement.
Shiatsu Massage for Sciatica Pain

Deep Suiatsu Massage for Chronic pain
In our sports medicine based curriculum, we emphasize that sciatica is rarely a local issue of the leg; it is the “alarm” of a silent dysfunction occurring elsewhere in the kinetic chain. If we see sciatica merely as a condition to be treated with localized rubbing, we risk overlooking its mechanical origins in lumbar instability or pelvic torsion.
To effectively treat this condition, a practitioner must start visualizing the three-dimensional relationship between the lumbar discs, the sacral plexus, and the deep rotators of the hip. In RSM's Shiatsu Massage Course, we teach that effective therapy requires a distinct shift in strategy: moving away from aggressive friction and toward the precise, stabilizing mechanics of shiatsu.
The Mechanical Origins of Sciatica
To understand why shiatsu is effective, we must first map the terrain. The sciatic nerve is the largest nerve in the body, originating from the L4 through S3 segments of the lower back. It bundles together and travels beneath, or sometimes through, the piriformis muscle before descending down the leg. Because of its size, it is uniquely vulnerable to entrapment.
Commonly, sciatic pain arises from two primary mechanical failures. First, a herniated disc can chemically irritate the nerve root. Second, and often misdiagnosed, is compression in the gluteal region. When the piriformis becomes tight due to pelvic instability, it strangles the nerve. In both scenarios, the body responds with a protective muscle spasm. This creates a hypoxic environment where tension accumulates, causing the patient to enter a “pain-spasm-pain” cycle.
Why Standard Massage Often Fails to Provide Relief
While standard Swedish protocols often prescribe long, gliding strokes, my experience suggests that this approach often backfires. When a nerve is inflamed, it becomes mechanosensitive. Aggressive gliding strokes or deep shearing forces, common in generic deep tissue massage, can stretch the nerve or drag irritated tissue across it.
This mechanical agitation triggers a sympathetic nervous system response. Instead of relaxing, the muscles tighten further to protect the threatened nerve. This leads to a “rebound effect” where the client feels temporary relief followed by an intense spike in pain hours later. Deep tissue work, if applied without anatomical precision, can actually increase the inflammation around the nerve root.
The Shiatsu Massage Advantage
In contrast, shiatsu utilizes perpendicular, static pressure. This distinction is critical for sports medicine applications. When we apply vertical pressure to a specific point and hold it, we avoid the shearing forces that aggravate the nerve. Physiologically, this sustained compression stimulates mechanoreceptors, sending a signal to the central nervous system to lower muscle tone.
This creates a neurological reset. By accessing the parasympathetic state, shiatsu lowers the systemic threat level. As the tension in the external rotators melts away, the physical space around the sciatic nerve increases. We are not forcing the tissue open; we are signaling the nervous system to let go. This leads to sustainable sciatica relief without the risk of micro-trauma.
Assessing the Back and Pelvic Kinetic Chain
Before a single point is pressed, we must assess the structural reality of the client. At RSM, we look for the “silent saboteur.” Is the sciatica driven by an anterior pelvic tilt which jams the lumbar facets? Or is it a result of a leg-length discrepancy?
For instance, if a client presents with pain in the right leg, I often evaluate the left hip. If the left gluteus medius is weak, the right side may be overcompensating, causing the right piriformis to become chronically tight. Treating the pain on the right without addressing the instability on the left is a futile effort. Our massage strategy is always dictated by this functional assessment.
Protocols for Sciatica Relief: The Bladder Meridian
Once the assessment confirms the source, the shiatsu protocol begins at the origin. The Bladder Meridian mirrors the pathway of the spinal nerves.
- BL23 (Shenshu): Located at L2, this point addresses the lumbar plexus roots in the lower back.
- BL25 (Dachangshu): Located at L4, this is a primary site for addressing low back instability.
We apply deep, sinking pressure here. The goal is to separate the erector spinae muscle from the spinous process, reducing the compressive load on the vertebral discs. By softening the lumbar fascia, we indirectly reduce the hydraulic pressure within the disc, allowing the nerve root to “breathe” and providing immediate relief.
Addressing Deep Gluteal Pain and the Piriformis
The transition from the lumbar spine to the hip is where the battle is often won or lost. We utilize specific points to release the hip rotators.
- GB30 (Huantiao): This is the most critical point for sciatica. Located deep in the gluteal muscles, it provides direct access to the piriformis.
- GB31 (Fengshi): Located on the lateral thigh, releasing this point helps reduce tension in the iliotibial band.
When working on GB30, we use the elbow to apply gradual pressure. We wait for the tissue to yield. If we are patient, we can feel the deep fascicles of the piriformis relax, physically lifting the compression off the nerve. This targeted release offers significant pain relief by addressing the specific point of impingement.
Distal Decompression of the Sciatic Pathway
The kinetic chain continues downward. The sciatic nerve travels down the posterior thigh, sandwiched between the hamstring muscles. Chronic tension here can tether the nerve.
- BL40 (Weizhong): Known as the “Command Point” for the back, releasing the popliteal fascia at the knee helps free the tibial division of the nerve.
The pressure here must be broad and careful. By releasing the hamstrings and the calf muscles, we reduce the traction on the nerve from below. This distal release is frequently overlooked in standard massage but is essential for full neural mobility and lasting relief.
Massage and Corrective Exercise Integration
Massage alone provides a window of opportunity, but it does not fix the architectural fault. Once shiatsu has reduced the acute pain and lowered the muscle tone, the client must engage in active rehabilitation.
If the sciatica was caused by a disc herniation, we prescribe extension-based exercises. If piriformis syndrome was the culprit, we must look at strengthening the gluteus maximus. At our academy, we teach students that shiatsu is the “setup,” and movement is the “finish.” The passive therapy calms the storm, allowing the active exercise to rebuild the structure.
The Holistic Path to Recovery
Treating sciatica demands a move away from generalized “rubbing” and toward specific, outcome-based intervention. By utilizing the static pressure of shiatsu, we respect the biology of the inflamed nerve. We bypass the body’s defense mechanisms, release the deep rotators, and restore the glide of the neural tissues.
This approach views the body not as a collection of parts, but as an integrated tensegrity structure. When we free the nerve, we do not just stop the pain; we restore the patient’s capacity to move. This is the essence of clinical massage: a blend of ancient technique and modern medical logic that delivers profound, lasting relief.
Understanding the Differences Between Orthopedic and Sports Massage

orthopedic Massage for cervical mobility
Many practitioners assume that applying deep pressure to an athlete qualifies as sports-specific work, while others view clinical rehabilitation as merely a slower version of a standard massage. In RSM's Sports Massage and Orthopedic Massage Courses, we teach that to treat a client effectively, a therapist must distinguish the specific goals, assessment protocols, and physiological intent behind these approaches.
The Scope of Sports Massage in Athletics
Sports massage operates primarily around the timeline of an athletic event. Its fundamental purpose is to optimize the athlete’s physical state for performance or recovery. We categorize this work based on when it occurs: pre-event, inter-event, post-event, and maintenance.
During a pre-event session, the goal is physiological arousal. We use up-tempo rhythm to stimulate the sympathetic nervous system and increase local blood flow. Conversely, post-event work focuses on down-regulating the nervous system to flush metabolic waste. In this context, the therapist does not stop to investigate a complex injury or chronic issue in depth. The priority is general system recovery rather than specific structural correction. If a therapist were to apply deep, sedative techniques before a race, it would lower muscle tone excessively, destabilizing joints and impairing performance.
The Medical Focus of Orthopedic Massage
Orthopedic massage stands in contrast to the generalized approach of sports-based work. It is a multidisciplinary approach focused on treating painful conditions and soft tissue injuries affecting the locomotor system. When a client presents with specific complaints, such as frozen shoulder or sciatica, general flushing strokes are insufficient.
This modality aligns closely with the medical field. The objective is to identify the root mechanical fault causing the pain and address it through precise manipulation. For example, treating plantar fasciitis requires an evaluation of the entire posterior kinetic chain. A restriction in the calf muscles often limits dorsiflexion, forcing the foot to collapse and loading the plantar fascia. To resolve this, we apply orthopedic massage therapy techniques to the restriction itself. By restoring the range of motion, the tensile stress on the foot decreases. This causal chain illustrates why this form of therapy is corrective; it requires the therapist to visualize functional relationships rather than just addressing the site of pain.
Distinctions in Assessment and Massage Techniques
The most significant divergence lies in the assessment phase. In a sports context, assessment is often visual and brief. However, in an orthopedic setting, the assessment determines the treatment. We utilize orthopedic tests to isolate structures and differentiate between muscle tears, bursitis, or nerve impingement.
Once the structures are identified, the massage techniques become highly specific. We do not apply broad pressure. Instead, we use targeted friction, mobilization myofascial techniques, or pin-and-stretch. These interventions aim to break down scar tissue and realign collagen fibers. Addressing a stuck layer of fascia requires a slow, shearing force to engage mechanoreceptors. Rapid movement would simply glide over the restriction.
Addressing Injury and Functional Movement
When dealing with an injury orthopedic in nature, the concept of movement is paramount. Pain creates compensatory patterns. A client recovering from an ankle sprain may develop hip pain because they avoid loading the injured leg. An effective treatment plan addresses these compensations.
We combine myofascial release with active movement. By having the client move a joint through its range while the therapist applies tension, we re-educate the nervous system. This helps the brain recognize the new, pain-free range of motion.
Below are the operational differences a therapist must recognize:
- Objective: Sports targets timing and performance; orthopedic targets pathology and dysfunction.
- Assessment: Sports relies on observation; orthopedic relies on specific testing.
- Technique: Sports utilizes rhythmic strokes; orthopedic utilizes specific friction and release.
- Outcome: Sports aims for readiness; orthopedic aims for restoration of function.
While the definitions are distinct, the practical application often requires integration. However, the methodology must be sound. Understanding these variables allows the therapist to select the correct tool, elevating the practice from a routine massage to a clinical intervention. Whether the goal is flexibility or rehabilitation, we must respect the anatomy to facilitate healing.
Clinical Mastery of Pressure Techniques in Trigger Point Massage

Trigger Point Massage Therapy Course
Novice therapists may view a muscular knot as a simple structural snag, a tangled ball of fibers that requires forceful eradication. This perspective often leads to treatments that are excessively aggressive, causing unnecessary bruising and sympathetic nervous system recoil. In our Trigger Point Therapy Training at RSM International Academy, we teach that effective remediation relies on physiological responsiveness rather than brute strength. To truly resolve myofascial dysfunction, a practitioner must understand the intricate balance between applying mechanical force and respecting the neurological feedback loop of the tissue.
Understanding the Trigger Mechanism
Before discussing treatment, we must understand the target. A myofascial trigger point is not merely a “tight spot”; it is a microscopic physiological disaster zone within a taut band of skeletal muscle. It represents a cluster of sarcomeres, which are the basic contractile units of muscle fiber, that have become stuck in a state of continuous contraction.
This sustained contraction creates a vicious cycle known as the “Energy Crisis.” The sarcomeres consume energy to maintain the contraction, but the tightness compresses local capillaries, restricting the blood supply needed to deliver that energy. This leads to a local hypoxic and acidic environment, sensitizing nociceptors and sending pain signals to the central nervous system. When we apply pressure to this area, the goal is to reverse this ischemia. By applying compression, we temporarily blanch the tissue. Upon release, a “reactive hyperemia” occurs: a flush of fresh, oxygenated blood that washes away inflammatory metabolites and allows the sarcomeres to disconnect.
Differentiating Active and Latent Trigger Types
In clinical practice, distinguishing between an active point and a latent trigger is essential. An active point produces spontaneous pain responsible for the client’s primary complaint, often generating referred pain patterns. For example, an active point in the infraspinatus often mimics deep shoulder joint pain.
In contrast, a latent trigger does not cause spontaneous pain. The client is usually unaware of its existence until the therapist performs palpation. Despite being silent regarding conscious sensation, these latent points restrict range of motion and alter muscle activation patterns. If left untreated, they often evolve into active points under stress. Identifying and treating these hidden areas is often the key to long-term pain relief and functional restoration.
The Physiology of Pain
One of the most frequent corrections I make during practical training involves the calibration of intensity. There is a prevalent myth that “no pain, no gain” applies to trigger point massage. This is dangerous. If the pressure levels are too high, the client’s body instinctively guards against the intrusion. This tensing of the muscle counteracts the therapy.
We utilize a pain scale of 0 to 10, aiming for a “satisfying pain” level around 7. This level allows the client to breathe through the sensation. If the sensation sharpens into a wince-inducing sting (an 8 or 9), the sympathetic nervous system activates, cortisol levels spike, and the tissue hardens. Sustained, calibrated force communicates with the muscle spindles, signaling the neuromuscular system to reduce tone. Therefore, the technique is as much about neurological re-education as it is about mechanical release.
Core Techniques for Effective Release
Once the point is located, the therapist must select the appropriate delivery method based on the muscle’s location and depth.
Static Compression
This is the most fundamental form of point therapy. The therapist applies increasing force perpendicular to the muscle fibers until the tissue barrier is met. This depth is held steady. As the tissue releases, the therapist follows the relaxation, sinking deeper. Bouncing or rapid poking irritates the nociceptors and fails to induce relaxation in the muscles.
Deep Stripping Massage
Stripping massage involves applying pressure along the length of the taut band. The therapist glides slowly from one attachment of the muscle to the other, moving at a pace of roughly one inch every three seconds. This is highly effective for elongating the sarcomeres and serves as an excellent preparation for static compression.
Pin and Stretch
This active release variation is highly favored in sports medicine. The therapist applies manual pressure to the trigger point while the muscle is in a shortened position. While maintaining contact, the therapist (or the client actively) moves the joint to lengthen the muscle. This mechanical action forces the muscle fibers to slide under the pressure contact, breaking up adhesions and rapidly restoring length.
Optimizing Point Pressure and Duration
The duration of point pressure varies based on tissue density. Standard protocols suggest holding for 7 to 90 seconds. However, rigid counting is less effective than feeling for the release. A skilled therapist waits for the “melting” sensation; a subtle softening of the nodule. Once this shift occurs, the pressure must be adjusted. Continuing to press on a released muscle causes irritation, while releasing too early renders the effort wasted.
Accurate Palpation
Blindly applying force is ineffective. Accurate palpation determines the success of the session.
- Flat Palpation: Used for muscles that can be pressed against a bone, such as the paraspinals or infraspinatus. The therapist slides cross-fiber to detect the ropy texture of the taut band and locates the tender nodule.
- Pincer Palpation: Used for muscles that can be lifted, such as the sternocleidomastoid or latissimus dorsi. The therapist grasps the muscle belly between thumb and fingers, rolling the fibers to detect the twitch response. This allows for precise isolation of specific points.
Clinical Application in the Kinetic Chain
At RSM, we emphasize that trigger point therapy should never be a static, isolated event. The body operates in chains. A trigger in the Vastus Lateralis may cause knee pain, but the root cause might be an inhibited Gluteus Medius.
Upper Body Application
Consider the Upper Trapezius, a common site for tension headaches. Treating the Trapezius alone is often insufficient. The Levator Scapulae and Rhomboids are frequently involved. Furthermore, if the Pectoralis Minor is tight, it pulls the scapula forward, locking the Trapezius in an eccentric strain. Effective trigger point massage must address the Pec Minor to relieve the strain on the upper back.
Lower Body Application
In the lower body, dysfunction in the Gluteus Medius often mimics sciatica. Because these muscles are covered by thick fascia, thumb pressure is often insufficient. The use of the olecranon (elbow) is necessary to generate sufficient force. However, the therapist must sharpen the angle to target the specific points precisely. Treating the Gluteus Medius often requires addressing the Tensor Fasciae Latae (TFL) as part of the lateral stability chain.
Achieving Long-Term Pain Relief through Movement
Treating the point provides a window of opportunity, but it does not fix the movement pattern that created the problem. To achieve lasting pain relief, the massage must be followed by movement re-education.
After the point release, the neuromuscular system needs to be reset. We immediately integrate active range of motion exercises. This teaches the brain that the new range of motion is safe. Without this step, the brain may revert to the old, guarded movement pattern, causing the trigger points to reactivate.
Common Mistakes and Specific Danger Zones
Recognizing errors is the first step toward clinical excellence.
- Chasing the Pain: Focusing solely on where the client feels pain is a rookie error. The source is rarely the site of the symptom.
- Excessive Force: Applying too much pressure induces a sympathetic response, causing the muscle to fight back.
- Ignoring Danger Zones: Anatomy is non-negotiable. The anterior neck (carotid artery), axilla (brachial plexus), and popliteal fossa (behind the knee) require extreme caution. For example, when treating the Quadratus Lumborum, pressure must be directed toward the spine, not vertically into the kidneys.
Elevating the Standard of Manual Therapy
The efficacy of trigger point massage lies in the details: the angle of entry, the calibration of force, and the integration with movement. It is the ability to distinguish between a structural limitation and a functional restriction caused by a myofascial holding pattern.
At RSM International Academy, our mission is to elevate the standard of manual therapy. Whether addressing an elite athlete or a chronic pain patient, the intelligent application of pressure is a powerful catalyst for healing. The transition from stiff, painful dysfunction to fluid movement begins with a single, well-executed point release.
Summary of Key Protocols
- Identify: Use functional assessment to locate the relevant taut band.
- Isolate: Differentiate between active and latent trigger points.
- Treat: Apply calibrated pressure (ischemic compression, stripping, or pin-and-stretch) within the client’s tolerance (7/10 pain scale).
- Mobilize: Integrate active movement to reset neuromuscular control.
- Educate: Provide aftercare strategies to prevent recurrence.
Shiatsu Massage for Pain Management

Deep Shiatsu Massage Course
It is a mistake to see traditional Japanese bodywork merely in the sense of energetic balancing. Such a view overlooks its potential role in clinical rehabilitation. In my experience training practitioners in RSM's Shiatsu Massage Course, I consistently find that the rigorous application of perpendicular static pressure offers a distinct mechanical advantage over friction-based modalities. When we analyze the physiological response of tissue under load, it becomes clear that this modality is not just about relaxation; it is a precise instrument for correcting structural dysfunction.
We must understand that pain is rarely an isolated event. It is the result of a kinetic chain failure. When a client presents with discomfort, the site of the symptom is often just the victim, not the culprit. By integrating anatomical logic with specific Japanese manual techniques, we can address the root causes of musculoskeletal restriction.
The Physiological Mechanisms of Shiatsu Massage
To truly master shiatsu, a therapist must move beyond simple memorization of points and visualize the relationship between fascia and the autonomic nervous system. Unlike Swedish or Deep Tissue protocols, which rely on gliding strokes that can trigger a defensive guarding response in inflamed tissue, this method utilizes sustained, vertical pressure.
This distinction is vital. When pressure is applied vertically and held without shearing force, it stimulates mechanoreceptors—specifically Ruffini endings—without aggravating the nociceptors (pain receptors) that react to friction. Consequently, the central nervous system receives a signal of safety. This leads to a rapid down-regulation of the sympathetic nervous system and an activation of the parasympathetic state.
In this state, muscle tone decreases, and local ischemia is resolved. The sustained compression forces blood out of congested tissue. Upon release, fresh oxygenated blood rushes in, flushing out metabolic waste. This “ischemic compression” principle is how massage facilitates recovery at a cellular level.
Integrating Shiatsu Therapy with Sports Medicine
At RSM, we teach this not as a mystical practice but as a clinical approach to soft tissue mobilization. The benefits of this integration are most apparent when treating athletes. An athlete’s body is often subjected to repetitive high-velocity loads, leading to dense fibrosis.
Standard massage therapy often attempts to break these adhesions through force. However, aggressive stripping can cause micro-trauma. In contrast, shiatsu therapy respects the body’s barrier. We apply pressure to the point of resistance and wait for the tissue to melt. This is the phenomenon of thixotropy, where the viscosity of fascia changes from a gel to a sol state under sustained load.
By utilizing body weight rather than muscular force, the therapist generates deep penetration that reaches the core of the hypertonic muscle without bruising the client. It is a sustainable model for both care provider and patient.
Managing Back Pain Through Structural Alignment
I frequently encounter cases of lumbar discomfort where the problem begins far from the spine. Back pain is frequently a compensatory price the body pays for stiffness in the hips or hamstrings. When the hamstrings are tight, they force the pelvis into a posterior tilt, flattening the lumbar lordosis and placing hydraulic pressure on the intervertebral discs.
Managing this condition requires more than rubbing the sore spot. We must release the tension in the posterior femoral muscles to allow the pelvis to return to neutral.
Specific protocols address the quadratus lumborum (QL) and the psoas major. The QL often becomes hyperactive to stabilize the spine when the core is weak. By applying precise thumb pressure to the lateral border of the QL, we can release the lateral traction on the lumbar vertebrae. Simultaneously, we must address the lower back from the anterior. The psoas muscle often creates an anterior pelvic tilt when shortened. Addressing these opposing forces restores the neutral alignment of the low back, providing long-term relief.
Targeting Chronic Conditions and Arthritis
Chronic inflammatory conditions present a unique challenge. In cases of arthritis or fibromyalgia, the patient’s pain threshold is significantly lowered. The dragging sensation of oil-based massage can overstimulate the skin’s sensory nerves, causing “rebound pain.”
Shiatsu bypasses this issue. Because the pressure is static, there is no friction to irritate the skin. This makes it an ideal therapy for chronic pain populations. We work proximal to the inflamed joint to reduce tension in the muscles crossing that joint, thereby increasing the joint space.
For example, with osteoarthritis of the knee, we release the tensor fasciae latae and calf muscles rather than pressing on the patella. This reduces compressive load during gait.
Manual Therapy for Headaches and Cervical Dysfunction
Upper crossed syndrome is ubiquitous due to modern computer use. This posture involves forward head carriage, increasing the load on cervical extensors. The resulting tension often manifests as tension headaches.
Treating this requires a dual focus: releasing the suboccipitals and opening the pectorals. The shoulders roll forward, shortening the pectoralis minor and compressing the brachial plexus. By opening the anterior chest wall with passive stretching and static pressure, we allow the scapula to retract. The headaches subside not because we rubbed the head, but because we corrected the cervical fulcrum.
RSM’s Approach to Lower Back Pain
At RSM, we look at the whole system: skeletal, muscular, and neurological. Musculoskeletal pain is rarely linear. A restriction in the ankle can cause a functional leg length discrepancy that creates shear force in the sacroiliac joint.
Massage therapists trained in this method learn to assess gait and posture first. If we treat the chronic lower back but ignore the collapsed arch in the foot, the issue will return. Joint pain is the signal; the kinetic dysfunction is the noise.
In a specialized pain clinic setting, we see patients with chronic central sensitization. The rhythmic nature of this modality provides a somatic anchor, creating an environment where the brain can “unlearn” guarding patterns. The care plan moves from acute symptom reduction to functional restoration. By respecting anatomical layers and working with the nervous system, we facilitate a structural reset. This is the essence of sports medicine-based pain management.
Developing Palpation Skills for Therapists

Clinical Palpation and manual therapy training
Students in our Orthopedic Massage Course may attempt to address a shoulder restriction by focusing on the glenohumeral joint, overlooking subtle fascial density in the pectoral girdle. Because they do not truly explore the tissue, they miss the story it is telling.
To truly master soft tissue therapy, a therapist must visualize the three-dimensional relationship between layers. When a therapist rushes this phase, they lose the neurological trust of the client’s body. Touch is not just a mechanism for delivery; it is a mechanism for gathering intelligence. If the sensory input from your hands is dull or distracted, your treatment plan will be generic. Therefore, the development of palpation skills is not optional; it is the foundation of all manual medicine.
The Role of Diagnostic Palpation in Clinical Assessment
In the context of sports medicine, there is a distinct difference between “feeling” a muscle and performing diagnostic palpation. The former is passive; the latter is interrogative. Diagnostic palpation requires a specific intent: you are looking for deviations in texture, temperature, tenderness, and tone. When a therapist approaches a clinical assessment, they must first understand that pain in one area is often the result of mechanical failure in another. For instance, lateral knee pain in a runner is rarely a local problem. It is frequently the compensatory price paid for a rigid hip capsule or a restricted ankle.
Consequently, diagnostic palpation serves as the bridge between the patient’s subjective report and the objective reality of their anatomy. If a practitioner skips this step, they are guessing. Guessing leads to ineffective treatment. Conversely, precise assessment allows the practitioner to map the dysfunction accurately. When you locate a patch of fibrotic tissue, you are identifying a potential disruption in the entire kinetic chain. This finding directs your treatment strategy, ensuring that you treat the cause rather than just chasing symptoms.
The effectiveness of massage therapy relies heavily on this initial data collection. If the assessment is flawed, the therapy will be misdirected. This is why we emphasize that palpation is continuous. It does not stop when the massage begins. Every stroke is an opportunity to re-evaluate the tissue response. If the tissue pushes back against your pressure, your palpation has just informed you that the nervous system is in a sympathetic state, requiring an immediate adjustment in depth or speed.
Palpation Guidelines for Precision and Depth
Developing high-level palpation skills requires adherence to specific mechanics. One of the most frequent corrections I make during practical training is adjusting the student’s body mechanics. If your shoulders are hiked or your wrists are rigid, your proprioceptors are dampened by your own tension. To feel the subtle vibrations and restrictions in a client’s tissues, your own hands must be relaxed and receptive.
Palpation guidelines often suggest a “less is more” approach, and this is anatomically sound. The sensory receptors in your fingertips – specifically the Merkel nerve endings – are most effective when not compressed by excessive force. If you press too hard immediately, you blanch your own fingertips, effectively blinding your sensors. Instead, you must “melt” into the layers.
We teach a concept of “sinking” rather than “pushing.” When you place your hand on the skin, you first acknowledge the cutaneous layer. You then wait for the tissue to accommodate your presence before sinking to the superficial fascia. Only after the superficial fascia yields do you sink further to the deep investing fascia and finally the muscle belly. This layered approach prevents the patient’s stretch reflex from firing. If you bypass the superficial layers and drive straight for the bone, the muscle spindle cells will detect a threat and trigger a contraction. This is the “fighting” sensation many novice therapists feel. They believe the muscles are tight, but in reality, they have created that tightness through aggressive entry.
Mastering the Seven-Step Palpation Method
At RSM, we respect structured learning protocols that reduce cognitive load for students while ensuring consistency. In osteopathic medicine, a widely recognized framework is the seven-step palpation method (often referenced by the acronym PALPATE: Position, Anatomy, Level, Purpose, Ascertain, Tweaking, Evaluate). Adapting this rigorous teaching method for the sports massage context helps therapists systematize their workflow. It transforms palpation from a random search into a logical checklist.
Here is how we integrate this structured approach into palpation tasks:
- Position (P): The therapist and client must be comfortable. If the client is fighting gravity to hold a limb up, their muscles will be active, masking the resting tone. We ensure the limb is fully supported so the target tissue is electrically silent.
- Anatomy (A): Before you touch, you must visualize. You are not just rubbing skin; you are projecting your mind’s eye through the layers. If you are palpating the shoulder, visualize the fiber direction of the supraspinatus passing under the acromion.
- Level (L): Determine the depth. Are you assessing the skin temperature (superficial), the fascial glide (intermediate), or the bony contours (deep)? Consciously shifting your “level” of attention changes what you perceive.
- Purpose (P): Why are you touching this specific spot? Are you looking for a trigger point? Are you checking for joint effusion? Touching without purpose is loitering. Every contact must have a clinical question behind it.
- Ascertain (A): This is the active phase of step palpation. You move the tissue or the joint to verify your hypothesis. If you suspect a restriction, you apply a shear force to ascertain if the tissue slides or if it is adhered.
- Tweaking (T): This refers to micro-adjustments. Maybe you need to change the angle of your pressure to get under the scapula border. These small tweaks often reveal the true pathology hidden by neutral positioning.
- Evaluate (E): Finally, you synthesize the data. Does the finding match the client’s complaint? If the client complains of sciatica but the piriformis is soft, you must evaluate other causes. This step closes the loop and leads to the treatment plan.
This seven-step palpation framework forces the student to slow down. By isolating each variable, the therapist avoids the common mistake of rushing to a conclusion. It ensures that when you do decide to treat a specific structure, you are doing so based on evidence gathered through a rigorous palpatory evaluation.
Refining the Sense of Touch
The transition from a novice to an expert lies in perceptual learning. Palpation is not merely a motor skill; it is a sensory processing skill. In the early stages of a career, a therapist might feel a “knot.” With years of practice, that same therapist feels the difference between a trigger point within the muscle fiber and a lipoma sitting on top of it. This distinction is critical because the treatments for those two entities are diametrically opposed.
We encourage students to engage in “blind” palpation tasks (exercises where vision is obscured). By closing their eyes, they remove visual distractions and force the brain to rely solely on somatosensory input. This heightens the sensitivity to texture and tension. When you remove vision, you stop looking at the skin and start seeing with your fingertips. You begin to notice the subtle drag that indicates a fascial adhesion or the slight increase in heat that suggests localized inflammation.
Furthermore, palpatory skills are enhanced by understanding the concept of “end-feel.” When assessing joint mobility or soft tissue length, the quality of resistance at the end of the range tells a story. A “bony” block suggests an articular limit. A “springy” block suggests a meniscal issue. A “leathery” restriction suggests capsular tightness. A massage therapist who can interpret end-feel through palpation can distinguish between a problem that needs stretching and a problem that needs a referral.
Osteopathic palpation concepts heavily influence our curriculum because osteopaths are trained to feel the “motility” or inherent motion of tissues, not just the mobility. While sports massage is generally more vigorous, incorporating this level of sensitivity allows for safer treatments. For example, before performing a deep release on the neck, a therapist should palpate the pulses of the vertebral artery. Ignoring these subtle signs can lead to injury.
Consistent practice is the only path to mastery. You cannot learn palpation from a textbook; you must feel hundreds of different bodies. Every client presents a unique topography. By constantly exposing your hands to these variables, you build an internal library of “normal” versus “abnormal.” This library becomes your greatest clinical asset. In the end, the skills of a therapist are defined by their ability to listen with their hands. Palpation is the intelligence that guides your tools. Without accurate palpation, you are working in the dark. With it, you are navigating the complex landscape of the human body with a map, capable of finding the root cause of dysfunction.
