
RSM Blog: Manual Therapy Techniques
Essential Skills for Future Massage Therapists

Trigger Point Therapy and Postural Assessment
The Importance of Advanced Anatomy and Knowledge
True clinical efficacy begins before a hand ever touches a patient. At RSM’s massage school here in Thailand, I emphasize that a map is useless if you do not understand the terrain. For students entering our program, particularly those with backgrounds in physiotherapy or athletic training, the study of the human body must go beyond memorizing Latin names. It requires a functional, three-dimensional understanding of how musculoskeletal systems interact.
Anatomy is the language of our profession, and a superficial grasp of muscle groups is insufficient for resolving chronic pain or addressing complex sports injuries. We teach our students to visualize the layers of tissue and the neural pathways involved in movement. This depth of knowledge allows a practitioner to distinguish between referred pain and local injury. Specifically, advanced anatomy and physiology enable a massage therapist to formulate effective treatment plans that address root causes rather than merely alleviating symptoms. When a practitioner possesses this understanding, the dynamic of the treatment room changes from a simple service exchange to a professional healthcare interaction.
Balancing Hard Skills with Clinical Precision
While theoretical understanding provides the map, hard skills determine our ability to traverse the landscape. In our training, these refer to the manual techniques and the quality of touch applied during a session. Palpation is the most critical tool in our arsenal. It is the ability to “see” with your hands, detecting subtle changes in tissue texture and tone often before the patient verbalizes them.
At our academy, we focus heavily on body mechanics. The longevity of a career in massage therapy depends on how well a therapist protects their own body while delivering force. We instruct students to use body weight rather than muscular strength, ensuring that deep tissue work is sustainable. Precision in applying pressure and the angle of entry are variables that must be controlled with exactitude. Effective massage techniques are not about how much pressure one can apply, but how intelligently one can apply it. This balance separates an amateur from a master.
Communication and Interpersonal Skills in Practice
Technical prowess means little if a practitioner cannot connect with the person on the table. Communication is the bridge between clinical assessment and patient cooperation. We often see students who are technically brilliant but struggle to articulate their findings, hindering the healing process.
Active listening is a vital competency. It involves hearing what the patient says regarding their history while observing non-verbal cues like guarding or grimacing. We must create an environment where the client feels heard. Clear verbal explanation is equally important; a therapist must translate complex medical concepts into language the patient understands.
Interpersonal skills extend to reading the room and adjusting one’s demeanor. Some patients require a calm presence to downregulate their nervous system, while others need motivation for rehabilitation. Adapting to these needs requires a high degree of emotional intelligence.
The Role of the Massage Therapist in Holistic Health
The modern healthcare landscape is shifting toward integrative care, where massage plays a central role alongside orthopedics and physiotherapy. We view the massage therapist not as a subordinate, but as a collaborator in patient health.
Professionalism encompasses everything from hygiene to boundary management. In a clinical sports setting, strict adherence to ethical standards is required to maintain a safe therapeutic container. Furthermore, a successful therapist must view their work through a lens of problem-solving. The ability to synthesize information from the intake and physical examination defines clinical reasoning. This cognitive process elevates massage therapy from a luxury service to a vital health intervention.
Elevating Your Massage Career and Business Acumen
To thrive in this field requires a commitment to lifelong learning. The field of sports medicine is constantly evolving, and the most successful massage therapists are those who remain curious. We encourage our students to view their initial training not as the end, but as the beginning.
A robust program provides the foundation, but experience builds the structure of a career. However, business acumen is often overlooked in traditional courses. Understanding how to manage a practice and retain clients is essential for sustainability. Even for those in clinics, understanding the business side ensures professional growth and allows the therapist to advocate for their value.
Why These Skills Matter for Your Clients
Ultimately, mastering these competencies serves the well-being of the people we treat. Clients come to us in pain, recovering from injury, or seeking performance enhancement. They trust us with their bodies.
When we combine anatomical knowledge with precise manual skills and professional ethics, we offer a service that is truly transformative. We help athletes return to their sport and office workers find relief. The impact of high-quality massage extends far beyond the hour spent on the table.
In the competitive landscape of wellness, these essential skills are the differentiator. Whether you are a physiotherapist looking to improve manual skills or a yoga instructor seeking a new avenue, the journey to mastery is ongoing. By focusing on these core areas – anatomy, technical precision, and communication – you become not just a technician, but a respected specialist in sports medicine therapy. The demand for highly skilled professionals is growing, and the future belongs to those willing to do the work.
Advanced Strategies in Massage Therapy for Chronic Pain Relief
Deep Tissue Massage for Chronic Pain Relief
Treating persistent suffering requires a rigorous application of sports medicine principles. At RSM International Academy, we often see students – many of whom are physiotherapists, doctors, or experienced bodyworkers – who are frustrated by traditional massage education. They come to our Remedial Massage Course seeking a deeper understanding of how to address the complex neurobiology of chronic pain.
We must move beyond the view that we are merely relaxing muscles. Instead, we are engaging with the body and its nervous system to alter how it perceives threat signals. Pain is an output of the brain, not just an input from the tissues. Therefore, our manual interventions must aim to downregulate this central alarm system, communicating safety rather than triggering a protective guarding response.
Effective Massage Therapy and Pain Management
The distinction between acute nociception and a chronic state dictates our clinical approach. If we treat a sensitized nervous system with the aggressive friction used for an acute injury, we risk further inflammation. Effective pain management requires selecting the correct modality for the specific presentation.
While Swedish massage is often dismissed in clinical circles as purely recreational, its utility in reducing sympathetic nervous system dominance is significant. By shifting the patient into a parasympathetic state, we create the physiological environment necessary for healing. Conversely, specific conditions require targeted work. We often identify a trigger point, a hyperirritable spot within a taut band of skeletal muscle. Applying ischemic pressure followed by a release allows for the perfusion of fresh, oxygenated blood, breaking the metabolic crisis sustaining the contraction.
However, a singular massage intervention is rarely a cure-all. We must look at the evidence critically to understand what works. An overview of current literature suggests that while the mechanisms are complex, the positive clinical outcomes regarding range of motion and psychological well-being are clear.
Addressing the Root of Chronic Pain
Structure dictates function. When a patient presents with muscle pain, we rarely look only at the site of symptoms. A structural imbalance in the kinetic chain often forces specific muscle groups to overwork. For example, restricted mobility in the thoracic spine often forces the cervical spine to compensate.
If we focus solely on the neck, we provide only temporary relief. The symptoms will return because the biomechanical root remains unaddressed. At RSM, I emphasize assessment before treatment. We observe gait, posture, and active range of motion to design massage sessions that are corrective rather than palliative. We are re-balancing tension relationships across the skeletal framework.
Integrating Evidence into Patient Care
The transition from short-term gain to long-term resolution depends on how we integrate manual therapy into the patient’s broader health strategy. Passive treatments create a window of opportunity during which the patient can engage in active rehabilitation.
A clinical review that included various manual therapies found that outcomes improved significantly when manual work was combined with exercise and education. We teach our students to view themselves as part of a larger medical team. Whether you are a yoga instructor or a physiotherapist, your role involves educating the patient on maintaining structural changes.
Therapeutic massage bridges the gap between medical necessity and holistic well-being. It is technical, precise, and rooted in anatomy. By constantly questioning and refining our understanding, we elevate the standard of care. The practitioner who understands the science of massage therapy is better equipped to offer true healing, restoring autonomy to patients who feel trapped by their condition.
Mastering Orthopedic Massage for Elderly Clients

Orthopedic Massage and dynamic postural assessment
At RSM International Academy, we apply the rigorous principles of sports medicine to every person we treat, regardless of athletic status. While we often associate biomechanics with elite athletes, these concepts are arguably more critical when applied to the aging population. The margin for error is smaller, and the impact of restoring mobility is profound. When treating the older generation, we are engaging in a complex negotiation with physiology that demands high-level expertise, not just a gentle touch.
Beyond Standard Geriatric Massage
There is a misconception that treating older adults requires a lack of technical precision. Geriatric massage is frequently taught as a simplified relaxation routine, but this fails to address the specific pathologies of aging. The biological reality of an eighty-year-old body involves sarcopenia and significant alterations in collagen. Connective tissue becomes dehydrated and less pliable, preventing fascia from gliding smoothly over muscle.
Applying orthopedic massage principles requires a shift in intent. We are not forcing length into shortened structures. In RSM’s Orthopedic Massage Course, students learn that effective massage is about strategy. We visualize dehydrated fascial layers and use slow, broad-contact pressure to encourage hydration. This approach respects the fragility of the capillaries while effectively addressing mechanical restrictions that relaxation techniques simply cannot reach.
Navigating Musculoskeletal Changes and Care
The cornerstone of working with this demographic is understanding musculoskeletal degeneration. Osteoarthritis often manifests as chronic pain and stiffness, but the root cause of discomfort is frequently the protective guarding of surrounding muscles. My approach involves down-regulating the nervous system to release this secondary tension first, providing immediate joint comfort.
A specialist understands that relieving the back pain of an elderly client might require releasing the hip flexors or addressing pelvic alignment. We must also consider the systemic effects of massage therapy. Circulation is often compromised in older adults. While increasing blood flow is one of the primary benefits of our work, we must modulate the volume of fluid moved to avoid overwhelming a compromised cardiovascular system.
Safety, Logistics, and Rehabilitation Feet
The logistical aspects of care are as vital as the manual techniques. We often utilize side-lying positions to reduce respiratory restriction and protect the cervical spine. Furthermore, we place a heavy emphasis on the extremities. The feet are the foundation of balance, and proprioception declines with age. We integrate specific rehabilitation feet protocols designed to stimulate nerve endings. By waking up sensory receptors, we do more than relieve soreness; we potentially improve stability and reduce fall risks for older clients.
Lymphatic Drainage Massage and Home Considerations
A frequent complication in aged care is edema. As activity levels drop, fluid accumulates in the lower limbs. Here, we often pivot to lymphatic drainage massage. This modality uses rhythmic, feather-light pressure to “invite” fluid movement, reducing the swelling that exacerbates joint pain.
Many graduates will also encounter patients who cannot travel. Home massage presents unique variables for the massage therapist, requiring adaptability to maintain ergonomics while treating clients in beds or armchairs. When delivering massage aged populations require consistency over intensity. Frequent, shorter sessions are often more effective than sporadic deep work.
The Role of the Specialist
The intersection of sports medicine and geriatrics is vital. An injury in a young athlete heals; in an elderly client, it can mark the start of a permanent decline. By applying the rigor of sports massage using assessment and functional goals, we change that trajectory.
Massage is not a luxury here; it is maintenance. We treat muscle pain to enable movement. If a client can move without pain, they remain active, preserving muscle mass and independence. Treatment plans at RSM are always focused on these functional victories. When we provide this level of care, we honor the resilience of the human form through exacting, expert practice.
Essential Skills for Sports Massage: A Guide for Therapists

Netherlands national team massage therapist chose RSM
True clinical efficacy begins where the textbook ends. At RSM International Academy in Chiang Mai, we operate on a fundamental truth: touching the human body is an act of profound responsibility. When we approach a table, particularly when working with high-level performers, we are not merely rubbing muscles. We are interacting with a complex, dynamic biological system. My experience in sports medicine has taught me that the gap between a competent practitioner and a master lies not in the number of certifications on the wall, but in the depth of their perception and the precision of their intent.
The defining characteristics of a world-class therapist are cognitive and tactile. In RSM’s Sports Massage Course, we teach students to understand the forces applied to the body during competition and how to reverse the trauma those forces create. This requires a specific set of competencies that blend scientific rigor with intuitive dexterity.
Understanding the Core of Sports Massage
The discipline of sports massage is often misunderstood as simply a “deep tissue” treatment applied to active individuals. In reality, it is a systematic manipulation of the soft tissues designed to focus on individual muscle groups relevant to a specific sport. The objective is function. A therapist must understand the biomechanics of a sprinter differently than those of a swimmer, as the sports context dictates the treatment plan.
We treat the body as a kinetic chain. If a pitcher complains of shoulder pain, we do not look only at the rotator cuff; we examine the hip rotation and the planting foot. This holistic view is what separates a sports massage session from a general spa experience. The work we do facilitates recovery, prevents injury, and enhances performance. It is a crucial component of an athlete’s training regimen, not a luxury add-on. To achieve this, the practitioner must possess a sophisticated understanding of how the body fails and repairs itself.
The Intersection of Anatomy and Physiology Skills
Foundational knowledge is non-negotiable. However, rote memorization is insufficient. A therapist must possess functional anatomy and physiology knowledge. You must know where the muscles attach, but more importantly, understand how they glide against neighboring structures and how they respond to fatigue.
When we discuss physiology skills, we refer to understanding the body’s internal chemistry and mechanical responses. For instance, understanding the difference between concentric and eccentric loading helps a therapist predict where micro-tearing is most likely to occur. If a runner engages in heavy downhill training, the eccentric load on the quadriceps is immense. Knowing this allows the therapist to anticipate the texture and tension patterns they will encounter before touching the client.
Furthermore, a nuanced grasp of physiology allows the therapist to discern when to apply circulatory techniques to flush metabolic waste versus friction to break down scar tissue. This is where technical knowledge translates into clinical results.
Technical Mastery Beyond Basic Massage Techniques
The hands are the primary diagnostic tools. At RSM, we emphasize that massage techniques are only as good as the sensitivity of the hands applying them. Palpation is the most valuable skill to possess.
We utilize a variety of modalities. Effleurage is often dismissed as basic, but in the hands of an expert, it is a powerful diagnostic sweep. In the application of distinct massage effleurage, the therapist establishes trust, warms the tissues, and scans for temperature differentials. It serves as the gateway to deeper work.
As we progress, techniques like deep stroking and petrissage become essential. Deep stroking must be applied with correct vector and intent; we are not just pushing down, we are elongating fibers. The ability to sink into the soft tissue without triggering a guarding response is an art form. These techniques skills must be adaptable. The pressure used for a pre-event flush differs vastly from the slow work required for post-event rehabilitation.
Why Assessment is Critical for Every Sports Massage Therapist
Assessment is not a preliminary step; it is a continuous process. A competent sports massage therapist assesses the client the moment they walk through the door, observing gait and posture.
Formal assessment skills involve specific range of motion (ROM) testing and orthopedic evaluation. Before treating a hamstring, we must know if the limitation is muscular, neural, or articular. The answers dictate the protocol. Assessment continues during the treatment as we evaluate the tissue’s response. Does the muscle tone drop? If the tissue fights back, the therapist must adjust immediately.
We also place immense value on verbal intake. We must discern patients’ preferences and pain history accurately. A skilled history-taking might reveal that lower back pain started after changing running shoes, pointing the assessment toward the ankles rather than the spine.
Tailoring Treatment for Athletes and Recovery
Athletes are a unique population. Their bodies are their livelihood. Consequently, the psychological component of the treatment is significant. When an athlete feels that the therapist understands the demands of their sport, the nervous system down-regulates, allowing for deeper healing.
Recovery strategies vary based on the training cycle. We often categorize our approach into three distinct phases:
- Maintenance: Addressed during regular training to prevent injury and reset resting muscle tone.
- Event-Based: Broken down into pre-event stimulation and post-event flushes to manage inflammation.
- Rehabilitation: Focused work on specific injuries to return the athlete to performance.
The performance of the athlete is the ultimate metric of our success. We must work in concert with the coach. Communication with the coach ensures that our manual therapy aligns with the physical loads being placed on the body.
Advanced Sports Massage Therapy Protocols
As a therapist advances, they move beyond general protocols and begin to treat specific pathologies. This is the realm of sports massage therapy where clinical reasoning becomes paramount. Conditions like plantar fasciitis or tendonitis require precise, localized interventions.
This often involves friction techniques to break down cross-linked collagen fibers. It requires a thorough understanding of the healing stages of tissues. Treating an acute sprain with deep friction is an error; treating chronic fibrosis with light pressure is equally useless.
The advanced therapist also understands the role of the nervous system. Techniques like proprioceptive neuromuscular facilitation (PNF) stretching rely on manipulating the body’s reflex arcs to induce relaxation in the muscles. This requires precise timing and clear communication.
The Role of Soft Tissue Manipulation in Sports
Soft tissue manipulation is the primary vehicle for change. In the context of sports, soft tissue includes muscles, tendons, ligaments, and fascia. Fascia envelops every structure in the body, and when it becomes adhered, it restricts movement globally.
Our massage skills must include myofascial release. This differs from standard massage as it involves a slow, shearing pressure that engages the barrier of the tissue resistance. It is not about sliding over the skin but engaging the deeper layers to create structural change. For the athlete, maintaining soft tissue health is synonymous with career longevity. Regular intervention keeps the tissues hydrated and mobile.
Integrating Orthopedic Massage Principles
To truly excel, one must incorporate orthopedic massage principles. This discipline bridges the gap between relaxation and medical treatment, focusing on correcting structural imbalances.
Orthopedic massage relies heavily on kinesiology. If a cyclist presents with knee pain, the orthopedic approach looks at the tension balance between the quadriceps and hamstrings and the tracking of the patella. We use specific testing to isolate the structures involved. The integration of these principles elevates the status of the massage therapist from a service provider to a clinician.
The Professional Evolution of Massage Therapists
Becoming an elite practitioner is a journey of constant evolution. Massage therapists who stagnate are those who stop asking “why.” At RSM, we instill a culture of curiosity. The field of sports medicine is always advancing; our understanding of physiology changes with new research.
Longevity in this career also requires self-care. The physical demands of performing high-quality massage therapy are high. We must apply biomechanics to our own bodies. If the therapist is injured, they cannot serve the client. Professionalism extends to ethics as well; maintaining boundaries and keeping accurate records of every assessment builds the trust necessary for high-level athletes to allow us into their inner circle.
Final Thoughts on Mastery
The path to mastery demands a synthesis of intellectual hunger and physical discipline. The skills needed for sports massage – from the nuance of massage anatomy to the precision of techniques, from the logic of assessment to the empathy required to understand a client – lay the foundation for a successful practice.
At RSM International Academy, we teach a philosophy of care. We teach our students to see the body as a marvel of engineering that requires respect and precise maintenance. We are guardians of movement, facilitating the human capacity to perform, recover, and excel. The hands can heal, but only when guided by a knowledgeable mind.
Shiatsu Massage for Anxiety Reduction: A Sports Medicine Perspective

Deep Shiatsu Massage Course
Anxiety is not merely a mental state; it is a profound physiological event. As the founder of RSM International Academy, I often perceive the somatic “noise” of a client before they even speak. It manifests as elevated resting tissue tone, shallow respiration patterns, and a nervous system stuck in a sympathetic loop. While talk therapy addresses the mind, bodywork – specifically the sustained, perpendicular pressure of shiatsu – addresses the hardware that the mind runs on.
In the Deep Shiatsu Massage Course at RSM’s school in Chiang Mai, we teach that effective health outcomes require understanding the biological mechanisms of touch. We do not view stress relief as a luxury, but as a necessary biological reset. This article explores the anatomical and neurological pathways through which this modality modulates the nervous system to lower stress and restore function. By bridging the gap between traditional wisdom and modern sports medicine, we can see how shiatsu can help recalibrate the body’s response to pressure.
How Shiatsu Can Help Regulate the Nervous System
The primary mechanism by which manual therapy affects mental state is through the autonomic nervous system (ANS). The ANS acts like a seesaw between two states: the sympathetic (fight-or-flight) and the parasympathetic (rest-and-digest). Chronic mental strain weights the seesaw heavily toward the sympathetic side, resulting in high cortisol levels and constant vigilance.
We utilize shiatsu to facilitate a shift back to the parasympathetic state. Unlike dynamic forms of bodywork that may stimulate blood flow through friction, this practice relies on static pressure. When a practitioner applies stable, vertical pressure to a specific point, it sends a clear, non-threatening signal to the brain’s safety receptors. This input down-regulates the sympathetic firing rate.
Research into the vagus nerve highlights why this approach is effective. The vagus nerve is the main data highway for the parasympathetic nervous system. Stimulation of mechanoreceptors in the connective tissue, particularly in the neck and abdominal regions often targeted in our sessions, can increase vagal tone. High vagal tone is correlated with the ability to recover faster after a stressful event. By mechanically signaling safety to the fascial network, we invite the brain to lower its guard.
Distinguishing Shiatsu Technique from General Massage
To the untrained eye, many bodywork modalities look similar, but the physiological intentions differ significantly. Swedish massage, for instance, often utilizes effleurage – long, gliding strokes designed to increase circulation and move lymph. While beneficial, this continuous movement can sometimes keep the sensory nerves active and alert.
Shiatsu technique is distinct in its use of stillness. We apply pressure perpendicular to the body surface and hold it. This “sustained pressure” allows the mechanoreceptors to adapt. Instead of bracing against a moving hand, the tissue realizes it is being supported and eventually releases its holding pattern.
This distinction is vital. A nervous system on high alert interprets rapid movement as potential danger. Stability, however, interprets as safety. By using body weight rather than force, shiatsu practitioners create a grounding sensation that anchors the client’s proprioception, helping them feel physically contained and secure. Unlike standard massage shiatsu offers a unique approach to boundary and depth. The practitioner sinks into the skin rather than sliding over it, reducing sensory noise and allowing for a deeper drift into a meditative state.
Mechanisms to Relieve Anxiety in Sports Medicine
In the context of athletics, mental distress is a performance killer. It ruins sleep quality, slows recovery, and increases the risk of injury due to poor coordination. Therefore, we view mental tension not just as an emotional hurdle, but as a physiological barrier to peak performance.
The physical manifestation of this state is often “guarding”; a subconscious contraction of structures to protect vital organs. This is why stressed individuals frequently report tight chests and rigid necks. The connection between somatic tension and emotional state is bi-directional: distress causes tension, and chronic tension signals the brain to remain distressed.
We can interrupt this loop by targeting specific areas known to harbor this protective tension, such as the trapezius or the diaphragm. When we achieve relief in these core areas, we lower the baseline “noise” of the nervous system. The individual may not even realize how much energy they were expending just to hold their posture until that rigidity is gone.
We also utilize acupressure points within our framework. Points such as Pericardium 6 on the inner forearm are not mystical buttons; they are areas rich in nerve endings that have a profound effect on the central nervous system. Accessing these points helps relieve anxiety systemically, rather than just treating a local symptom.
Strategies for Deep Relaxation and Recovery
For anyone seeking to improve their mental resilience, consistency is key. A single session provides a temporary reset, but regular treatments retrain the nervous system to default to a calmer baseline. We recommend integrating relaxation shiatsu into a broader recovery routine. This might look like scheduled sessions to manage strain accumulation or using simple pressure techniques during moments of acute distress.
Evidence indicates that shiatsu helps release tension not just mechanically, but psychologically. The supportive touch provides a “container” for emotions that may be too difficult to verbalize. In our clinic, we often see patients experience an emotional release on the table, a sign that the body is finally feeling safe enough to let go of its vigilance.
When tracking effectiveness, we look at various anxiety-related measures. Subjective reports of sleep quality are usually the first to improve. Clients often report falling asleep faster and staying asleep longer. We also look for improvements in range of motion and a decrease in resting heart rate. These objective metrics help us validate the subjective feelings of calm.
Why Shiatsu is a Distinct Intervention
It is important to view this as a complementary intervention. While shiatsu massage is powerful, it works best alongside other treatments if an individual is dealing with clinical depression or severe panic disorders. We always encourage a multidisciplinary approach.
However, as a standalone tool, it is unparalleled. One of the unique aspects we emphasize at RSM is the diagnosis of “Kyo” (deficiency) and “Jitsu” (excess). Anxiety symptoms often present as “Jitsu” in the upper body and “Kyo” in the abdomen. Our goal is to disperse the excess and tonify the deficiency. This balancing act draws energy down from the racing mind and anchors it in the Hara (belly), producing a state of deep relaxation.
Chronic pain and mental distress often feed into each other. By breaking this cycle with shiatsu, we address both. The release of endorphins manages the pain, while the vagal stimulation manages the mental state. Evidence shows that shiatsu benefits quality of life by addressing the somatic roots of our emotions.
Through the skilled application of touch, we can help reduce anxiety and return to a state of balance. Whether utilizing this for anxiety treatment support or general well-being, the modality offers a non-invasive, drug-free option for regulating the internal environment. Muscle relaxation leads to mental relaxation, proving that the path to recovery often begins with the simple, grounding power of touch.
How to Maintain Professional Boundaries in Therapeutic Practice

Dynamic Myofascial Release and postural assessment
The precise application of force to a hypertonic muscle requires more than anatomical knowledge; it requires trust. When a client enters a treatment room, they hand over the autonomy of their physical body. This transaction is profound. It rests entirely on a framework that is often invisible until it is broken.
In sports medicine, we work with the raw mechanics of the human body. We touch what hurts, and for many clients, the relief creates an immediate bond. However, the efficacy of our work depends on the structure surrounding it. Without rigid edges, the container leaks. As practitioners, we often focus on the “how-to” of technique, yet understanding the architecture of the therapeutic relationship is equally critical. At RSM International Academy in general, and with special emphasis in our Remedial Massage Course, we teach students how to establish clear parameters, and avoid the risk of compromising the treatment, the client’s safety, and our own longevity.
The Vital Role of Professional Boundaries
In manual therapy, professional boundaries are the defined limits protecting the space between the professional’s power and the client’s vulnerability. This is not a wall to keep people out; it is a perimeter defining where the work happens.
New students often believe that being “caring” means saying “yes.” They extend sessions because the client is in pain or listen to deep personal traumas to offer support. While the intention is benevolent, the result is a degradation of standards. When a therapist operates without a clear boundary, the dynamic shifts. The client may unconsciously view the therapist as a friend or subordinate. In sports medicine, where we require compliance with rehabilitation protocols, maintaining authority is essential. The onus is always on the therapist to manage the dynamic, regardless of the client’s behaviours.
Why We Maintain Appropriate Professional Boundaries
We maintain appropriate professional boundaries not because we are indifferent, but because we are professionals. The safety of the client is paramount. Touch triggers the release of oxytocin and can surface suppressed emotions. If the therapist reciprocates this personal intimacy, it confuses the purpose of the session.
Furthermore, boundaries are the primary defense against burnout. A therapist who absorbs the emotional weight of every client or fails to separate their personal life from their clinical practice will not last. The physical demand of sports massage is high; adding emotional exhaustion is unsustainable. Consider the athlete who pushes limits. They might push you to work deeper than is safe. By holding firm, you model a respect for limits they often lack. The boundary itself becomes a therapeutic tool.
Defining Work Boundaries in a Clinical Setting
Structure provides safety. When work boundaries are ambiguous, anxiety fills the gap. Clients want to know exactly what to expect. This begins before the client ever gets on the table.
Your hours are your hours. If you finish at 6:00 PM, treating a client at 6:30 PM is not a favor; it is a breach of the structure. It signals that your time is negotiable. Once a client believes your time is negotiable, they may begin to believe your clinical decisions are also negotiable.
We teach our students to consider the physical environment. The treatment room should be neutral. Personal photos or political items can alienate clients or invite conversations that distract from treatment goals. Setting these parameters early is efficient. If you are clear about cancellation policies and communication methods from the first intake, you reduce the friction of future interactions.
The Intersection of Personal Care and Therapy
There is a distinct difference between being friendly and being a friend. Clients often unload their stresses, which is natural. However, the therapist must navigate this with care.
We are not psychotherapists. While we offer a compassionate ear, we must not actively engage in counseling. When a therapist offers life advice, they step outside their scope of practice. Moreover, the conversation should never flip. The therapist should not unburden their own problems onto the client. Using session time to discuss your own concerns reverses the flow of care.
Creating a separation between your internal state and your external performance is a skill requiring training. You may be having a terrible day, but those emotions must be shelved when you enter the treatment room. If you are distracted by your own narrative, you will miss the subtle cues of the body under your hands.
Navigating Complex Boundaries
Certain scenarios test boundaries frequently. Physical draping is non-negotiable. It protects the client’s modesty and the therapist from allegations. Even if a client claims they are comfortable without it, you maintain the standard because it protects the professional relationship.
Social interaction requires similar discipline. In a community like Chiang Mai, you will see clients in public. You do not initiate the interaction. If they greet you, respond briefly. Never discuss their treatment in public. Digital communication also requires setting boundaries. Direct all scheduling to official channels. This reinforces that the relationship is professional, not social.
Balancing Work and Emotional Investment
To sustain a career, you must examine your workload. There is a finite amount of energy you can expend. Work-life balance is a physiological necessity for a manual therapist. If you are depleted, your mechanics falter.
Therapists often over-identify with a client’s recovery, feeling they have failed if the client is not healed. This enmeshment is unhealthy. You provide the stimulus; the client’s body provides the response. Maintaining professional distance allows you to see the clinical picture clearly. Objectivity is a requirement for excellence.
Strategies to Maintain Integrity
Implementing this requires a deliberate approach to working habits. We must be proactive rather than reactive.
Here is a practical framework:
- Codify Your Policies: Have written documents regarding cancellations and conduct. This moves the boundary from a personal rejection to a policy enforcement.
- Ritualize the Process: Wash your hands before and after every session. It signals the beginning and end of the contact.
- Uniform: Wear a uniform to create a visual distinction between “you the person” and “you the therapist.”
- Refer Out: Recognize when a client’s needs exceed your skill set.
We must also consider interactions with colleagues and staff. Healthy clinic dynamics depend on mutual respect. Confidentiality extends to peers; we discuss cases for learning, not entertainment.
Setting professional standards is an ongoing process. When we consider reasonable boundaries, we look at the long game. We want to treat clients for decades. Your preferences regarding clients or hours are valid. You do not have to be everything to everyone.
The barrier gives the river its power. By holding the line, you channel your energy directly into the treatment, ensuring every session is safe and effective. This is the discipline of the professional. This is the standard of RSM.
Myofascial Release in Orthopedic Practice and Treatment Protocols

Dynamic Myofascial Release for posture correction
Modern sports medicine has advanced our understanding of fascia as a primary source of proprioception, force transmission, and frequently, chronic dysfunction. I teach students in RSM’s Orthopedic Massage Course that treating the musculoskeletal system without addressing the fascial network is mechanically counterproductive, as the restricted tissue continues to anchor bones and muscles in their dysfunctional positions regardless of external adjustments.
For the clinician, the integration of targeted soft tissue manipulation into standard rehabilitation protocols is not optional; it is essential for resolving complex pain patterns.
Understanding Myofascial Pain and Myofascial Tissues
The human body relies on the gliding potential of its internal structures. Myofascial tissues surround and penetrate every muscle, bone, nerve, and organ, creating a three-dimensional matrix that provides structural integrity. When trauma, inflammation, or poor posture occurs, this tissue dehydrates and thickens. The resulting restrictions exert pressure on pain-sensitive structures, often reaching up to 2,000 pounds per square inch.
This phenomenon creates myofascial pain that does not follow standard dermatomal patterns. A patient may present with symptoms mimicking radiculopathy, yet diagnostic imaging reveals no nerve compression. The culprit is often a densification of the fascia which traps nerve endings and restricts blood flow.
In my clinical experience, recognizing these restrictions distinguishes a technician from a true healer. Pain acts as a complex signal. It is rarely isolated to the site of the symptom. A restriction in the thoracolumbar fascia, for example, often manifests as pain in the hip or shoulder due to the interconnected nature of the kinetic chain. Effective management requires looking beyond the site of complaint to the tension lines transmitting the strain.
The Efficacy of Myofascial Release Therapy in Treatment
To effectively resolve these issues, we employ myofascial release therapy. This modality differs significantly from traditional massage. While massage often targets the belly of the muscle to increase circulation, this specific treatment applies sustained pressure into the myofascial restrictions to eliminate pain and restore motion.
The mechanism involves the piezoelectric effect. When a therapist applies gentle, sustained pressure, the mechanical energy converts to heat energy, changing the viscosity of the ground substance within the fascia from a solid to a gel state. This phase change allows the tissue to elongate and release the trapped structural components.
We frequently see orthopedic conditions such as plantar fasciitis, frozen shoulder, and chronic low back pain respond rapidly to this approach. By addressing the soft tissue environment, we reduce the load on the skeletal system. A joint cannot move freely if the distinct fascial layers surrounding it are adhered together. Consequently, mobilizing the joint without releasing the surrounding tissue often leads to a recurrence of symptoms.
Integrating Manual Therapy and Physical Therapy
There is a symbiotic relationship between manual therapy and active rehabilitation. In many clinical settings, physical therapy focuses heavily on strengthening and range of motion exercises. While these are vital, attempting to strengthen a muscle bound by fascial restriction can exacerbate dysfunction.
At RSM, we advocate for a sequenced approach. The manual therapy component prepares the body for movement. Once the pain levels decrease and the restrictions yield, the patient can engage in physical therapy exercises with correct biomechanics. If a patient attempts to strengthen a shoulder girdle while the pectoralis fascia is glued tight, they will only reinforce a compensatory movement pattern.
This integration is particularly relevant for occupational therapists and those working in postoperative rehabilitation. Scar tissue is fascia that has healed haphazardly. Unless this tissue is remodeled through direct intervention, it remains a permanent barrier to full functional recovery. We must view the physical body as a tensegrity structure where a change in tension at one point inevitably affects the whole.
Addressing Physical Limitations Through Release Work
The technique used in release work requires patience and tactile sensitivity. We teach our students that you cannot force the fascia; you must wait for it to yield. This distinction is crucial for pain relief. Aggressive input often triggers a protective muscle spasm, halting the therapeutic process.
When treating chronic conditions, we look for the trigger points which may be referring pain to distant areas and causing significant motor dysfunction. Release work deactivates these points by flushing out sensitizing chemicals and restoring local perfusion.
The physical demand on the patient is minimal during the session, yet the physiological shift is profound. Patients often report a sensation of “letting go” or a deep ache that feels productive. This indicates that the release techniques are engaging the collagenous barrier effectively.
Clinical Application of Myofascial Release
In the realm of sports medicine, the margin for error is small. Athletes require optimal tissue compliance to perform at high velocities. I have observed that incorporating myofascial release into maintenance protocols significantly reduces the incidence of non-contact injuries.
The evidence supporting fascial manipulation has grown substantially. Recent articles and research highlight the role of fascia in force transmission and proprioception. It is no longer viewed as a passive container but as an active, sensory organ.
We consider myofascial release techniques a fundamental pillar of modern medicine and rehabilitation. Whether the goal is returning an elite athlete to the field or helping an office worker manage neck pain, the principles remain the same. We must restore the fluid dynamics and sliding surfaces of the body.
The pain associated with orthopedic issues is often multifaceted. By treating the connective tissue system, we address the root cause of the structural imbalance rather than merely managing the symptoms. This comprehensive approach ensures that treatment outcomes are durable, restoring not just the absence of pain, but the presence of functional freedom.
Effective rehabilitation demands this level of detail. As practitioners, our ability to palpate and treat these restrictions defines the quality of care we provide. The future of orthopedic care lies not just in the mechanics of the joint, but in the health of the fabric that holds it all together.
A Clinical Overview of Common Myofascial Release Techniques

Dynamic Myofascial Release for Dorsal Scapulae Nerve
The Physiology of Fascial Restriction
The human body is an architectural marvel of tension and compression, held together by a pervasive network known as fascia. While early anatomists frequently discarded this connective tissue to expose organs and bones, we now understand that fascia is a sensory-rich organ enveloping every nerve and vessel. In RSM’s Myofascial Release Course, we emphasize that treating the musculoskeletal system without addressing the fascial web is futile.
Fascia relies on hydration and movement. Healthy tissue consists of collagen fibers in a lattice structure, bathed in lubricating hyaluronic acid. When trauma occurs or a body remains static, this lubricant becomes viscous. The layers adhere to one another, creating densification that restricts range of motion and alters force transmission. Pain is often the final signal of this dysfunction. By the time a client reports chronic pain, the fascial architecture has likely been compromised for months. The goal of any manual therapy intervention is to restore the slide and glide potential between these layers, applying specific inputs to change the viscosity of the ground substance and relax surrounding muscles.
The Role of the Therapist in Myofascial Release
Clinical outcomes depend heavily on the palpation skills of the therapist. A generic protocol cannot account for the unique densifications in a specific patient’s body. I teach my students that their hands must act as listening devices. The practitioner must differentiate between a hypertonic muscle, which is a neurological state, and fascial stiffness, which is a structural change in the tissue.
In a clinical setting, myofascial release involves applying low-load, long-duration stretch into the complex. The practitioner waits for the tissue to yield, a phenomenon known as creep. This relies on the piezoelectric effect, distinct from deep tissue massage which focuses on metabolic clearance. The approach we teach prioritizes the barrier concept; engaging the tissue just to the point of resistance without triggering a defensive stretch reflex. This respect for the barrier facilitates a true release of tension.
Active Release and Sports Performance
While static pressure is effective, the demands of sports medicine often require dynamic interventions. Active release protocols differ from passive treatments by incorporating patient movement. This logic is grounded in functional anatomy: muscles and fascia operate in coordinated chains, not isolation.
During an active release session, the practitioner applies tension to a specific structure while the patient moves the limb through a range of motion. This physically shears the fascial layers apart, breaking down fibrotic adhesions. Simultaneously, it educates the nervous system. By forcing the brain to control the movement while the tissue is under tension, we rewrite motor patterns. This method is valuable for high-level athletes requiring optimal performance, bridging the gap between passive manual therapy and active movement.
Integrating Self-Myofascial Release Tools
Daily maintenance is essential for long-term health. We encourage patients to utilize self-myofascial release (SMR) as a preventative measure. While the market is flooded with devices, the efficacy of these tools depends entirely on proper application.
Common instruments include:
- Foam Rollers: For large surface areas like the quadriceps and latissimus dorsi.
- Massage Balls: For targeting specific trigger points or smaller groups like the gluteus medius.
- Massage Sticks: For manual pressure control on calves and necks.
The objective is not to bruise the skin but to identify restriction and apply sustained pressure.
The Mechanics of Foam Rolling
Foam rolling is often performed incorrectly. Rapid rolling acts like a rolling pin on dough; it flattens but rarely changes structure. Effective rolling utilizes autogenic inhibition. When the user finds a tender spot, they must pause and hold for 30 to 90 seconds. This sustained pressure stimulates the Golgi tendon organs, signaling the muscle spindle to relax. Only after this neurological reset should the user begin small shearing motions to address the fascial layers. It is not a warm-up, but a preparation for the warm-up.
Precision Work with a Massage Ball
A massage ball offers distinct advantages due to its smaller surface area, allowing penetration into deeper layers. For areas like the plantar fascia or subscapularis, a large roller is ineffective. Using a ball against a wall creates a fulcrum, useful for the upper trapezius where gravity creates tension. The user uses body weight to modulate intensity, mimicking a therapist’s pressure. However, understanding anatomical landmarks is crucial to avoid compressing nerves or bone.
Understanding Positional Release Protocols
Not all release techniques rely on direct pressure. Positional release, often associated with Strain-Counterstrain, is an indirect method effective for acute pain. The theory is that the body is stuck in a protective spasm. Instead of stretching the tight muscle – which might trigger contraction – we move the joint into a position of ease.
By shortening the affected muscle and holding it for roughly 90 seconds, we reduce proprioceptive activity. This silence allows the central nervous system to reset the resting tone. Upon returning the limb to neutral, the relief is often immediate. This subtle technique underscores that force is not always the answer.
Differentiating Trigger Points from Fascial Adhesions
It is vital to distinguish between general fascial tightness and trigger points. Treating trigger points requires focused ischemic compression to cut off local blood supply, then releasing it to encourage a flush of oxygenated blood.
Myofascial release therapy, by contrast, addresses the connective tissue matrix. While these issues often coexist, the clinical reasoning differs. I teach that treating the trigger point without addressing the surrounding fascial tension is a temporary fix. If the casing of the muscle remains shrunken, the trigger point will likely return. Comprehensive treatment addresses both the neurological trigger and the structural container.
The Mental Component and Rehabilitation
We cannot discuss physical release without acknowledging the emotional component. Fascia is innervated by the autonomic nervous system. It is not uncommon for patients to experience an emotional release during a session. We treat the physical manifestation of stress, but must respect the connection to the psychological state. When the tissue releases, the patient enters a state of parasympathetic dominance where healing occurs.
Furthermore, release is only the first step. Once range of motion is restored, it must be stabilized. Rehabilitation integrates with manual therapy by assigning corrective exercises to load the tissue in its new state. This convinces the nervous system that the new range is safe. Manual therapy opens the door; movement must walk through it to ensure pain relief lasts.
Clinical Efficacy and Education
The field of sports medicine is evolving. Strategies for mfr (myofascial release) once considered fringe are now central to recovery. However, efficacy relies on practitioner education. It is easy to learn a technique, but difficult to learn when to apply it. We see students with many modalities but lacking the diagnostic framework to choose the right one. The “release” is only as good as the assessment.
Conclusion: A Philosophy of Movement
The pursuit of health is about resilience. Fascia is the medium through which we experience physical reality. When it is healthy, we move with grace; when compromised, we feel trapped. By mastering the various release techniques available – from subtle positioning to deep shearing – we assist the body in returning to balance.
At RSM International Academy, we combine the art of palpation with the rigor of sports medicine. We believe understanding the “why” is as important as the “how.” Through this, we empower practitioners to provide lasting solutions, ensuring every patient has the opportunity to move without restriction.
How to Develop a Professional Massage Routine: Going Beyond Basic Techniques
Remedial Massage and sports medicine
Understanding the Foundation of Massage Therapy
I see many therapists struggle not with the quality of their touch, but with the cohesion of their sequence. They possess excellent individual skills but lack the connective logic to bind them into a seamless experience. Developing a routine requires you to think like an engineer as much as a healer. At RSM massage school here in Thailand, students learn how one muscle group connects to the next and how the application of pressure in one area affects the tension in another.
The goal of massage is rarely just relaxation; it is the restoration of function. Therefore, the routine you develop must prioritize safety and efficacy. A simple routine executed with profound anatomical knowledge will always outperform a complex routine performed with vague intent.
The Anatomy of Effective Massage Techniques
To construct a coherent routine, one must first categorize the tools available. The hands are capable of a vast array of mechanical inputs, but in a professional context, these usually fall into specific categories of techniques. The most fundamental of these is effleurage. This gliding stroke serves as the introduction and the conclusion of most sequences. It allows the therapist to spread massage oils evenly, assess the temperature and texture of the tissue, and accustom the recipient to touch.
Effleurage is not merely about spreading oil; it aids venous return and lymphatic drainage. When performing a hand effleurage, the direction must always be centripetal, moving toward the heart, to support the circulatory system. This is a non-negotiable rule in sports medicine.
Following the initial warm-up, the routine typically progresses to petrissage. This technique involves kneading, rolling, and lifting the soft tissue. Petrissage is essential for mobilizing muscle fibers and increasing local circulation. It addresses the “belly” of the muscle and is particularly effective in areas with higher muscle mass, such as the quadriceps or the back.
Within a professional sequence, one might also employ circular friction. This is a more targeted approach used to address adhesions or trigger points. It requires precision. The therapist applies pressure to a specific point and moves the skin over the underlying structure, rather than sliding over the skin.
The transition between these strokes dictates the quality of the massage. You begin with superficial effleurage to warm the tissue. You deepen the pressure gradually, introducing petrissage to mobilize the fluids. Only once the tissue is pliable do you apply deep friction. After the specific work is complete, you must reverse the gradient, returning to lighter strokes to flush the area. This bell-curve structure is the hallmark of a professional massage session.
Structuring the Back and Neck Sequence
The posterior chain is often the centerpiece of a full-body routine. The back presents a large surface area and houses the spinal column, making it a critical region for nervous system regulation. When structuring a back massage, the therapist should generally work from the lumbar region up toward the thoracic and cervical areas, following the direction of the erector spinae muscles.
A standard professional protocol might look like this:
- Initial Contact: Establish contact and apply lubrication broadly across the entire back surface.
- General Warm-up: Use effleurage alternate hands (shingling) to cover the length of the spine, warming the paraspinal muscles.
- Specific Mobilization: Transition to hand petrissage on the lateral aspects of the back, specifically the latissimus dorsi.
- Deep Work: Apply circular friction or thumb pressure along the laminar groove to address tension in the erectors.
- Integration: Conclude with long, sweeping effleurage strokes connecting the neck to the sacrum.
The neck requires a modification of pressure and intent. The cervical spine is delicate, and the muscles here – the upper trapezius, levator scapulae, and suboccipitals – are often laden with tension. In this area, we reduce the broad movements and focus on precision. High velocity or heavy pressure is dangerous here. Instead, we use slow, controlled traction.
When treating the neck, the therapist must ensure the recipient feels secure. We often suggest supporting the occiput with one hand while the other performs the specific work. This duality – support and treatment – is vital for the cervical region.
Mastering Pressure and Flow
One of the most common questions I receive from students is about pressure. How deep is too deep? The answer lies in the response of the body. Pressure is a conversation, not a monologue. If you force your way into the tissue, the body will push back.
Developing a professional routine means learning to generate pressure from your core, not your small joints. A massage therapist who relies on grip strength will burn out quickly and risk injury. At RSM, we teach biomechanics before we teach complex strokes. You must lean your body weight into the stroke, keeping your joints stacked and your spine neutral.
Flow is the result of confident transitions. In a professional massage, the therapist never breaks contact unexpectedly. If you need to move from one side of the table to the other, you maintain a point of contact. This provides a sense of continuity for the recipient.
Flow also refers to pacing. A sports massage designed for pre-event preparation will have a brisk, rhythmic pace to excite the nervous system. Conversely, a recovery session will use a slower, heavier cadence. Your routine must adapt its tempo to the goal of the therapy.
Positioning the Recipient for Optimal Results
Technique is rendered useless if the client is not comfortable. The environment and the positioning of the recipient set the stage for the entire treatment. This includes the temperature of the room, the quality of the table, and most importantly, the use of bolsters and draping.
For a back massage, a bolster placed under the ankles takes the tension off the hamstrings and lower back. Without this, the lumbar spine may remain in lordosis, preventing the lower back muscles from fully relaxing. Draping is both an ethical and a functional concern. It protects the client’s modesty and keeps them warm. A cold body will not relax; the muscles will shiver and contract, making deep work impossible.
The choice of massage oils or creams also plays a role here. A professional routine requires a medium that offers enough glide for effleurage but enough drag for tissue manipulation. If the skin is too slippery, you cannot engage the fascia; if it is too dry, you will irritate the skin.
Why Technique Alone Isn’t Enough
A technician may be able to replicate a sequence of massage techniques, hitting every muscle group in the correct order, and yet the session may feel mechanical and cold. A therapist, on the other hand, imbues the routine with presence and adaptability.
In my years of practice, I have found that the best routines are those that allow for improvisation within a structure. You might have a plan to treat the legs, but if you find significant restriction in the hamstrings, you must be willing to alter your time management. A rigid adherence to a plan ignores the reality of the body on the table.
Massage therapy is a dynamic interaction. We are not working on machines; we are working on living, breathing organisms. The routine is merely a map. You are the guide.
We must also consider the concept of “pain” in a professional context. Generally, pain is a signal of damage, but in deep tissue or sports therapy, there is often a sensation of “good pain” or therapeutic discomfort. It is the therapist’s responsibility to distinguish between the two. Sharp, electrical sensations are warning signs to stop. Dull, aching sensations that subside with breath are usually indicative of tension release.
Finally, we cannot discuss developing a routine without discussing the sustainability of the therapist. Giving high-quality treatments requires physical and mental stamina. If your routine places undue stress on your thumbs or lower back, you will shorten your career. Professional development involves analyzing your own ergonomics to ensure longevity. We encourage our students to practice self-care, including proper hydration and receiving wellness treatments themselves.
Developing a professional routine is an iterative process. It begins with the basics: anatomy, safety, and fundamental strokes like effleurage. It evolves through practice, feedback, and a deepening understanding of physiology. At RSM International Academy, we provide the scientific foundation, but the artistry of the routine comes from the dedication of the therapist. By respecting the anatomy and listening to the tissue, you build trust. This is the path to professional excellence.2
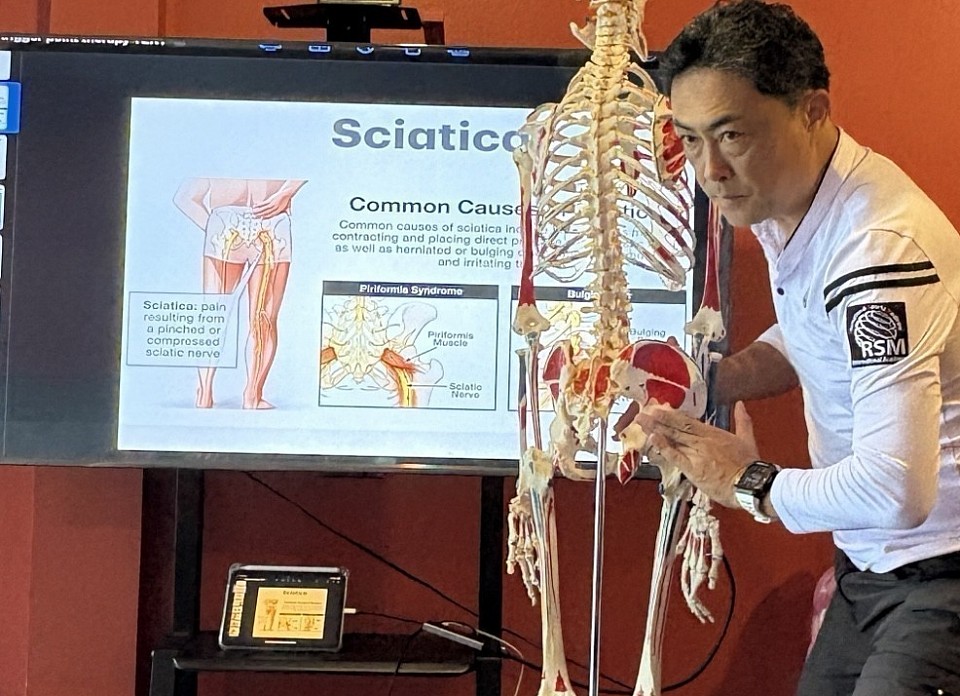
Trigger Point Massage for Chronic Pain

Trigger Point Masaage for Scapula Mobility
Identifying Trigger Points in Soft Tissue
A taut band of skeletal muscle fibers represents a physiological failure at the microscopic level. At RSM International Academy, we emphasize that effective manual therapy requires visualization of this underlying pathology. Many practitioners rely on intuition. However, a true clinical approach demands precision.
A trigger point is defined as a hyperirritable spot within a taut band. This spot is painful on compression and often produces referred symptoms. When we palpate a patient, we search for this specific textural anomaly. It feels distinct from surrounding healthy tissues. Healthy fibers yield; compromised areas feel like rigid nodules.
In RSM’s Trigger Point Therapy Course, we distinguish between active and latent points. An active nodule causes spontaneous discomfort, affecting the client constantly. Conversely, a latent nodule only produces sensation when external pressure is applied. Both types restrict movement and weaken the structure. Therefore, a comprehensive assessment scans for both to ensure long-term health.
The Physiology of Chronic Pain and Muscle Tension
To treat a condition effectively, one must understand its origin. The mechanism behind these “knots” is best explained by the “Integrated Hypothesis.” This theory postulates that dysfunction begins at the neuromuscular junction, forcing muscle fibers to contract continuously.
Inside the muscle, sarcomeres – the basic units of contraction – become locked. This sustained contraction compresses local blood vessels, restricting circulation. Consequently, the area suffers from hypoxia (lack of oxygen). This acidity sensitizes nerve endings, sending pain signals to the central nervous system. Simultaneously, the contraction depletes adenosine triphosphate (ATP), the energy molecule required for relaxation. The muscles remain tight because they lack the energy to release. This metabolic crisis is often the root cause of chronic pain.
Addressing Referred Symptoms and Pain Patterns
A confusing aspect for patients is the displacement of symptoms. The location where they feel the ache is rarely the source. This is known as referred pain. For instance, a headache behind the eye often originates from a trigger point in the neck. Treating the head offers no relief; treating the neck resolves the issue. This diagnostic capability separates a clinical massage therapist from a recreational practitioner.
We map these patterns to predict where the primary dysfunction lies. There are also “satellite” points that develop in the referral zone. If the primary point remains untreated, these satellites activate, expanding the area of problems. Successful treatment requires identifying the primary generator of the signal.
Treatment Strategies for Lasting Relief
At RSM, I constantly reinforce anatomical visualization. Blindly rubbing a sore area is inefficient and potentially dangerous. We often encounter nerve entrapment alongside muscular tension. A tight piriformis muscle can compress the sciatic nerve, creating symptoms that mimic a herniated disc, known as piriformis syndrome. Differentiating between structural spinal issues and soft tissue entrapment changes the therapy course.
We utilize several strategies to deactivate nodules and restore function:
- Ischemic Compression: Applying sustained pressure to flush the tissue and reset the neuromuscular loop.
- Deep Stroking: Stripping the length of the taut band to mechanically lengthen sarcomeres.
- Muscle Energy Techniques (MET): Using active contraction against resistance to lower tone via neurological inhibition.
This is point therapy in its most clinical form. It is not about relaxation; it is about restoring mechanical capacity.
Integrating Trigger Point Therapy into Rehabilitation and Recovery
Deactivating the nodule is only the first step. Musculoskeletal pain is often a symptom of poor posture or imbalance. Therefore, we must look at the entire kinetic chain. If a muscle is tight, its antagonist is likely weak. Restoring the full range of motion at the joint prevents the sarcomeres from locking up again.
Massage therapy serves as a catalyst. It opens a window where the body is mobile. The patient must utilize this window to retrain movement patterns. The body has an innate ability to repair itself once obstacles are removed. By eliminating the constant neural noise of trigger points, we allow the system to reset.
At RSM, our goal is to elevate the profession from the spa to healthcare. By understanding the physiological mechanisms of trigger point formation, we provide a specialized massage technique that fundamentally changes the quality of life for those suffering from tension and immobility. The transition from pain to performance begins with the skilled hands of an educated therapist.
Essential Shiatsu Massage Etiquette Guidelines and Massage Standards

Sports Massage for chronic pain
At RSM International Academy, our Shiatsu Massage Course is approached through the lens of sports medicine and functional anatomy. However, we also see etiquette as a framework that establishes safety, trust, and therapeutic efficiency. When a client understands the expectations of the clinic, the nervous system settles. This down-regulation of the sympathetic nervous system allows the massage to be far more effective.
I have spent years refining clinical protocols to ensure that every treatment delivers measurable results. A successful session requires collaboration between the client and the practitioner. By adhering to specific standards, you ensure that the focus remains entirely on rehabilitation and recovery.
Why Being Fully Clothed Matters in Shiatsu
One of the most distinct features of this modality is that the receiver remains fully clothed during the session. Unlike oil-based modalities where skin-to-skin contact is necessary, Shiatsu relies on compression, mobilization, and stretching.
Clothing provides friction. This friction is essential because it allows the therapist to stabilize a limb or apply a specific vector of force without slipping. If you were to wear slippery synthetic fabrics or attempt this on bare skin without oil, the practitioner would struggle to maintain the precise leverage required to manipulate the fascia.
Clothing choices directly impact the quality of the massage. We recommend wearing loose-fitting, comfortable cotton attire. Sweatpants and a t-shirt are ideal. Tight yoga pants can impede blood flow, and denim is too restrictive for passive stretching. Arriving with the correct attire demonstrates a respect for the biomechanics of the therapy. It allows us to work through the full kinetic chain without stopping to adjust drapes.
Navigating Massage Etiquette and Communication
Effective massage therapy relies heavily on a continuous feedback loop. Many clients believe that being a “good client” means remaining silent, even when they are in pain. This is a misconception that can hinder the treatment.
Pain causes muscle guarding. When the brain detects a threat, it signals the muscles to contract. If the pressure applied during a massage triggers this guarding reflex, the technique becomes counterproductive. You are essentially fighting the practitioner.
We encourage a clear dialogue regarding sensation. There is a clinical difference between “therapeutic discomfort” – the feeling of a knot releasing – and “injury pain.” You must communicate this distinction to your massage therapist immediately.
Common Etiquette Questions for Your Therapist
New clients often have uncertainties regarding the logistics of a massage. Uncertainty creates tension, so we aim to answer these questions proactively.
- Should I arrive early? Yes. Arriving 10 to 15 minutes early allows you to decompress. Rushing into the clinic elevates your heart rate. If you jump onto the table in a “fight or flight” state, the first portion of the massage is wasted trying to bring your baseline down.
- What about tipping? In a medical setting, tipping is not expected in the same way it is in a spa. However, in many massage contexts, it is a standard expression of gratitude. The primary focus of an RSM graduate is clinical outcome, not gratuity.
- Hygiene Protocols: In a sports medicine context, we work in close proximity. We request that clients arrive with clean socks or bring a fresh pair. This protects the health of the practitioner. If you are coming from a workout, a shower is necessary to create a sanitary environment for the massage.
Professional Boundaries and Modesty
The relationship between a client and a therapist is strictly professional. It is a therapeutic alliance designed to resolve physical dysfunction. While Shiatsu is performed clothed, eliminating the need for professional draping in the traditional sense, the concept of boundaries remains.
We respect your physical space and autonomy. In scenarios where Shiatsu is integrated with other modalities that require disrobing, draping protects both the client’s privacy and the practitioner’s professionalism. Proper massage protocols ensure that only the area being worked on is exposed. This protects modesty and maintains clinical integrity.
Even within a clothed modality, modesty preferences vary. Some clients are uncomfortable with abdominal work (Ampuku) or gluteal compression. A skilled practitioner will always ask for consent before working on sensitive zones. It is your right to refuse or modify any part of the treatment.
The Physical Environment and Electronics
The massage room is a controlled environment designed to minimize sensory input. This allows the brain to focus on internal signals.
Cell phones should be silenced. A vibrating phone is just as distracting as a ringing one. It pulls the mind out of the parasympathetic state and back into the reactive world of notifications. For the duration of the therapy, the outside world must wait. This rule applies to the therapist as well. You should expect your practitioner to be fully present, with no distractions from their own devices.
Respect Enhances Recovery
Ultimately, guidelines regarding behavior are about maximizing the health benefits of the interaction. When a client respects the therapist and the therapist respects the client, the therapeutic alliance is strengthened.
We see this clearly in the results at RSM International Academy. Clients who prepare properly, communicate clearly regarding pressure, and respect the boundaries of the clinic consistently show faster recovery rates. By following simple standards, such as removing socks if they are dirty, arriving on time, and communicating openly, you elevate the massage from a mere service to a collaborative health intervention.
Whether you are an elite athlete or someone seeking relief from chronic pain, understanding these etiquette guidelines ensures that every session moves you closer to your physical goals.
Manual Therapy Versus Orthopedic Massage: Defining Clinical Pathways

Orthopedic Massage for Cervical Mobility
Students in RSM International Academy’s Orthopedic Massage Course frequently encounter ambiguity regarding the boundaries of clinical bodywork. Specifically, the distinction between manual therapy vs orthopedic approaches often causes confusion. While both disciplines share techniques, they differ significantly in educational background, regulatory scope, and anatomical focus.
At RSM, we treat the separation between relaxation and medical-grade rehabilitation as a gradient. Understanding where skills overlap ensures that the patient receives appropriate care. It allows a practitioner to communicate effectively with physical therapists and other healthcare providers to optimize outcomes.
Defining the Umbrella of Manual Therapy
Manual therapy acts as a broad classification rather than a singular technique. It encompasses any clinical intervention where a practitioner uses their hands to assess and treat body structures. Physical therapists, osteopaths, chiropractors, and massage therapists all utilize forms of manual therapy.
However, the specific application depends on the provider’s license. Manual physical therapy involves a combination of soft tissue mobilization and specific joint manipulation to restore arthrokinematics. Conversely, orthopedic massage generally stays within the realm of soft tissue manipulation.
This distinction dictates the treatment plan. If a patient suffers from restricted range of motion, the therapist must identify if the block is articular or myofascial. A physical therapy diagnosis often points toward joint-specific interventions. In contrast, orthopedic massage targets the elasticity of the musculature surrounding that joint.
Clinical Approaches in Massage Therapy
Massage therapy in an orthopedic setting differs from standard spa treatments. It is strictly outcome-based. The therapist assesses the soft tissue to identify adhesions or hypertonicity contributing to the client’s complaint. Manual therapy offers targeted clinical results only when the practitioner understands the underlying physiology.
Massage therapists specializing in this field use techniques like friction and neuromuscular therapy. While deep tissue is a common term, orthopedic massage is more precise. It targets specific structures. For example, treating a rotator cuff injury requires understanding the fiber direction of the supraspinatus. The therapist applies tension to the tissue to assist in collagen remodeling.
We emphasize that orthopedic massage does not force a joint back into place. Instead, it creates an environment where the joint can function correctly. By reducing tension in the agonist and antagonist muscles, the therapist reduces compressive forces. Consequently, mobility improves without high-velocity manipulation.
Physical Therapists and Joint Mobilizations
Physical therapists operate with a wider diagnostic scope, emphasizing pathology and post-surgical protocols. They assess the spine and peripheral joints to identify structural dysfunction. This diagnosis directs the treatment.
In clinical practice, physical therapy integrates active exercise with passive manual interventions. Joint mobilizations are a critical component here. These involve skilled passive movements applied to a joint at varying speeds. Grade V mobilizations, or manipulations, involve a high-velocity, low-amplitude thrust.
Legal restrictions usually reserve these thrust techniques for physical therapists, chiropractors, and osteopaths. We teach students to recognize when a client requires this level of intervention. If a client has a structural block, soft tissue work alone may fail. Referring the client to a physical therapist becomes the ethical choice, enhancing the massage therapist’s reputation for safety.
Mechanisms of Pain Relief and Decreased Inflammation
The primary driver for seeking therapy is pain. Understanding the neurophysiology of pain relief is essential. Manual therapy stimulates mechanoreceptors within the joint capsule. This input overrides nociceptive signals, effectively closing the “gate” to pain.
Decreased inflammation is another benefit. By improving fluid dynamics, manual interventions help flush metabolic waste. Orthopedic massage addresses pain caused by ischemia, or lack of blood flow. Sustained muscle contraction restricts circulation. Specific compression forces blood out of hypertonic tissue. When released, fresh blood rushes in, flushing out inflammatory cytokines.
These physiological changes prove that massage is a biological interaction, not a placebo. However, the practitioner must dose the treatment correctly. Excessive pressure can increase inflammation, while insufficient pressure may fail to stimulate a response.
Differentiating Techniques and Sports Medicine
The difference between these fields is most visible in the selection of techniques. A physical therapy session often consists of brief manual work followed by significant corrective exercise. The manual portion prepares the body for load.
In contrast, an orthopedic massage therapy session usually dedicates the full duration to manual manipulation. This allows for a thorough address of the kinetic chain. If a runner has knee pain, the massage therapist has time to treat the foot, calf, and hip.
My background in sports medicine influences our curriculum. Sports injuries involve high-force loads that differ from the general population. In this context, the lines often blur. Physical therapists manage rehabilitation protocols and return-to-play decisions. Massage therapists manage recovery and tissue quality.
Rehabilitation is a continuum starting immediately after injury. Manual therapy addresses different needs at each stage. Lymphatic drainage aids acute swelling, while friction prevents scarring in the sub-acute phase.
A Collaborative Future
Ethical practice requires acknowledging our limits. Massage therapists assess dysfunction but do not diagnose medical conditions. We do not manipulate the spine with thrust techniques. Ignoring these boundaries puts patients at risk.
Ultimately, the distinction serves the client. Manual therapy provides the framework for hands-on care. Physical therapy uses it for structural diagnosis and rehabilitation. Orthopedic massage therapy uses it for soft tissue restoration.
We believe the future of treatment lies in integration. When a patient receives joint mobilization from a physical therapist and soft tissue release from an orthopedic massage therapist, recovery accelerates. By understanding sports medicine and joint mechanics, you become an indispensable part of the healthcare team. This technical excellence is the goal at RSM International Academy.
How to Avoid Injury During Massage Training

Proper Posture during Massage Sessons
Training to become a manual therapist is an athletic endeavor. Many students enter the field believing that empathy and strong hands are the only requirements for success. However, without a rigorous understanding of biomechanics, a student’s career can end before it truly begins. At RSM’s massage school here in Thailand, we view our students as athletes of the upper extremity. Just as a sprinter must learn running mechanics to prevent hamstring tears, a therapist must learn proper body mechanics to prevent burnout.
Injury rates in this industry are unacceptably high. Studies suggest a significant percentage of therapists leave the profession within the first five years due to work-related pain. This attrition is the direct result of poor training habits formed early in the educational process. We approach this problem through the lens of sports medicine. By understanding the anatomy of the practitioner, we can engineer a way of working that is sustainable, effective, and safe.
Understanding Body Mechanics for Long-Term Career Success
The term “body mechanics“ defines how a practitioner applies force to a client. Proper mechanics are about physics. The goal is to generate pressure using the largest muscle groups and the weight of the body rather than the small, fragile muscles of the hands and arms.
New students often rely on their intrinsic hand muscles to dig into tissue. This leads to rapid fatigue. Conversely, a seasoned expert generates force from the core and legs. They lean into the stroke. This transfers energy through a stacked skeletal structure. The bones bear the load rather than the muscles.
In massage, the kinetic chain begins at the feet. Force is generated from the ground up. If a therapist stands with locked knees, the chain is broken. Consequently, the therapist must compensate by pushing with the shoulders. This isolation causes strain. We teach students to adopt a “lunge” or “fencer’s stance.” This stable base allows the therapist to shift their weight forward and back. The movement comes from the legs and hips. The arms remain relatively static; they act as tools of transmission rather than engines of force.
The Anatomy of Common Injuries in Massage Therapy
To prevent injury, one must understand exactly what structures are at risk. Common injuries in this field are rarely acute. They are cumulative trauma disorders resulting from repetitive movements performed with slight deviations.
The Thumb and CMC Joint
The carpometacarpal (CMC) joint of the thumb is the most frequently injured site. This saddle joint allows for incredible range of motion; however, that mobility comes at the cost of stability. When a therapist presses directly into tissue with a hyper-extended thumb, the CMC joint sustains massive compressive forces. Over time, this wears down the articular cartilage and leads to osteoarthritis.
Wrist Pathology
The wrist contains the carpal tunnel. When a therapist works with a flexed or extended wrist, the pressure within this tunnel increases. Combined with the vibration and force of massage, this compression irritates the median nerve. This manifests as Carpal Tunnel Syndrome.
Shoulder and Rotator Cuff
Shoulder pain often stems from “hiking” the shoulders. When a therapist is tense, they unconsciously raise their shoulders toward their ears. This activates the upper trapezius. Chronic tension here alters the mechanics of the glenohumeral joint and can lead to impingement syndrome.
Why Massage Therapists are Athletes
We treat the training process at RSM International Academy with the same seriousness as elite sports training. Massage therapists engage in physically demanding work that requires endurance. A typical session involves hundreds of lunges.
Recognizing yourself as an athlete changes your mindset. An athlete prioritizes rest. If a pitcher feels a twinge in their elbow, they stop throwing. Similarly, a student learning massage must recognize that pain is a warning signal.
Overuse syndrome is the enemy. It occurs when tissue damage exceeds the rate of tissue repair. In the early stages of learning, the body is adapting to new stresses. Tendons adapt slower than muscles. Therefore, students must pace themselves. Pushing through pain establishes a cycle of inflammation.
Protecting the Thumbs and Wrists During a Massage Session
The hands are the primary tools of the trade. Protecting them is non-negotiable. We emphasize specific techniques to shield the small joints of the hand from excessive load.
Stack and Brace
A vital technique for deep pressure is reinforcing the thumb. Never use a single thumb to apply deep pressure. Instead, place your other thumb directly on top of the working thumb to brace it. This technique distributes the force. The bottom thumb acts as the sensor. The top thumb provides the structural support. This reduces the shear force on the CMC joint.
Use Alternative Tools
The thumbs should not do all the work. We train students to utilize the forearm and the elbow. The elbow is an incredibly powerful tool. It allows the therapist to apply deep pressure to large muscle groups without placing any stress on the wrists.
Neutral Wrists
Maintaining a neutral position is critical. A neutral wrist is straight; it is aligned with the forearm. When applying pressure, the force should travel in a straight line through the radius and ulna bones. Deviating from this neutral position creates torque at the wrist joint. This shears the soft tissues and increases the risk of tendinitis.
The Role of Neutral Position in Injury Prevention
Injury prevention relies on maintaining natural curves of the spine. When a therapist leans over a table, there is a tendency to round the thoracic spine and crane the neck forward. This “head-forward” posture places immense strain on the cervical extensors.
To avoid injury, the therapist must hinge at the hips. The spine remains straight. The bending motion occurs at the hips, not the waist. This hip hinge engages the powerful glutes to support the torso. It spares the smaller erector spinae muscles of the lower back. We continuously correct student posture to ensure this hip hinge becomes second nature. It is vital to practice good posture until it is automatic. Failing to maintain good posture during a session compromises the entire skeletal structure.
Self-Care Tips for Students and Professionals
Professional longevity requires a proactive maintenance strategy. Self-care tips are mandatory protocols for anyone serious about this career. The body requires maintenance to function at a high level.
Hydrotherapy
Contrast hydrotherapy is a simple method for increasing circulation and reducing inflammation. After a day of working, alternating between hot and cold water helps flush metabolic waste products. The cold constricts blood vessels which reduces inflammation. The heat dilates them and brings fresh blood to the area.
Targeted Stretching
Stretching must be specific. Massage therapy involves repetitive flexion of the fingers. Therefore, the flexor muscles of the forearm become tight. Regular stretching of the wrist flexors helps maintain balance. Extend the arm with the elbow straight. Gently pull the fingers back. However, one must also strengthen the extensors to correct the muscular imbalance.
Hydration
The fascia requires hydration to slide efficiently. Dehydration makes fascia sticky. This increases friction within the therapist’s own body. Drinking adequate water ensures that the tissues remain pliable.
How We Teach Safe Practice at RSM International Academy
At RSM, we integrate safety into every practical lesson. We do not teach a technique without simultaneously teaching the body mechanics required to execute it safely.
Our instructors observe the student’s stance first. If the stance is poor, the technique is flawed. We correct the foundation first. We also emphasize the mental aspect of prevention. Students are taught to scan their own bodies while working. Are my shoulders raised? Am I holding my breath? This proprioceptive awareness allows the therapist to make micro-adjustments.
Balancing Strength and Flexibility for the Therapist Body
Strength is a component of safety that is often overlooked. A massage therapist needs a strong core. The core muscles act as a transmission belt for force. If the core is weak, the force generated by the legs leaks out before it reaches the arms. The lower back takes the hit.
We encourage students to engage in resistance training. Exercises that target the posterior chain are particularly beneficial. These muscles counteract the forward-leaning posture of the work. Flexibility is equally important, but it must be balanced. If the joints are too loose, they lack stability. Therapists with hyper-mobile joints must focus on strengthening the muscles around those joints.
Recognizing Pain Signals and Prevention Mindset
Pain is not always a sign of damage, but it is always a request for attention. In a training environment, students often ignore minor aches. We challenge this narrative. Reporting pain is a sign of professional maturity.
When a student reports pain, we analyze their mechanics. Usually, the issue is traced back to a specific technical error. Correcting the mechanics usually eliminates the discomfort. If the pain persists, we implement injury rehabilitation protocols immediately.
The ultimate goal is to instill a habit of prevention massage within the therapist’s lifestyle. This means receiving therapy regularly. Self-care massage addresses the specific tension patterns that develop from giving massage. It also serves as a critical educational tool. We encourage students to view their career in decades. Prevent future issues by investing in the body today.
A Sustainable Path Forward
At RSM International Academy, we are committed to graduating therapists who are resilient. We believe that pain should not be the price of empathy. By adhering to strict biomechanical principles, prioritizing self-care massage, and treating the body with the respect due to an elite athlete, students can build a career that is enduring.
Quick Reference: The RSM Safety Protocol
- Warm-up: Always perform dynamic movements before a session.
- Check Your Stance: Use a lunge position. Drive from the legs.
- Neutral Wrists: Keep the wrist joint straight. Avoid extreme flexion.
- Protect the Thumbs: Never use a thumb unsupported. Brace it with your other thumb or use an elbow.
- Listen to Your Body: If it hurts, stop. Analyze your mechanics.
- Receive Work: Get regular massage to address your own compensatory patterns.
By following these guidelines, you ensure that your hands remain strong and your back remains healthy. The world needs skilled healers. It needs you to be healthy enough to do the work.
Establishing Rapport With Clients in Massage Therapy

Deep Tissue Massage for posture Correction
Effective manual therapy relies on more than anatomical knowledge or biomechanical precision. In RSM’s Deep Tissue Massage Course, we teach that the foundation of successful treatment lies in the relationship between the practitioner and the person on the table. Without trust, the nervous system remains guarded, making deep tissue work difficult and corrective manipulation less effective. Therefore, we emphasize that technical skill must coexist with the ability to connect.
I founded this school with the belief that sports medicine is a partnership. When an athlete enters our clinic, they are often in a state of vulnerability. If they do not feel safe, their muscles will not relax. Consequently, the first technique a therapist applies is not a touch, but a demeanor.
Building Rapport Through Clinical Competence
Trust is not abstract in a clinical setting; it is physiological. When a patient perceives competence, their sympathetic nervous system—the fight or flight response—begins to downregulate. This downregulation is essential for effective deep tissue massage. If the sympathetic nervous system remains active, muscle tone remains high, preventing the practitioner from accessing the deeper layers of soft tissue required to resolve chronic issues.
We define rapport as a state of harmonious understanding. In sports medicine, this understanding is rooted in the therapist’s ability to accurately assess and describe the problem. A client who feels heard and understood is a client whose body is ready to receive treatment. Conversely, a lack of clarity creates tension. If a therapist seems unsure, the body will instinctively resist.
This dynamic proves that building rapport is a clinical skill. It requires the same dedication to practice as learning the origin and insertion of the quadriceps. We train our students to view communication as a modality, adjusting their style based on the individual’s emotional state just as they would adjust pressure based on tissue density.
The Role of Active Listening in Massage
Communication happens in two directions. Too often, therapists focus on explaining findings rather than understanding the patient’s experience. The most critical tool for assessment is active listening.
Active listening extends beyond words; it involves listening to the tissue response. When you apply pressure to a trigger point, does the body recoil? Does breathing change? These are forms of communication. Ignoring them breaks the therapeutic bond. We instruct students to look for non-verbal cues. A clenched jaw or sudden holding of breath indicates the intensity is too high. Adjusting immediately shows the person on the table that you are tuned in to their experience.
Specific verbal confirmation is also necessary. Asking “Is this pressure acceptable?” allows the receiver to retain a sense of control. This agency is vital for comfort, transforming the session from a passive experience into an active recovery process.
Fostering Genuine Connections With Clients
Authenticity is the currency of any strong relationship. Patients can detect when a practitioner is reciting a script. To create genuine connections, you must bring your true self to the practice while maintaining professional focus. This means being present.
When I treat a high-level athlete, I show curiosity about their sport, training load, and recovery goals. This signals that I am invested in their outcome. A client who feels seen is more likely to return. Retention is driven by how a person feels during the transition moments—the greeting and the intake. These moments frame the physical work.
Setting Boundaries for a Healthy Therapeutic Relationship
There is a misconception that rapport requires becoming friends with those you treat. This is incorrect. Blurring lines can damage the therapeutic relationship. Professionalism requires clear structures. Setting boundaries actually increases comfort. When expectations are clear, anxiety decreases.
For example, maintaining strict draping protocols protects dignity. It signals that this is a medical environment. Personal boundaries also apply to conversation. While we want to be friendly, the focus must remain on treatment goals. If a conversation veers into uncomfortable topics, the therapist must steer it back to the work at hand.
This separation allows you to maintain longevity. If you absorb the emotional weight of every person you treat, burnout is inevitable. Establishing boundaries ensures that the tenth client you see in a week receives the same quality of attention as the first.
Why Rapport Matters in Sports Medicine Outcomes
Rapport is not just a “soft skill”; it is a clinical accelerator. A strong relationship fosters client compliance.
Rehabilitation rarely happens entirely within the clinic. We often prescribe corrective exercises or lifestyle modifications. If the person does not trust our expertise, they are less likely to follow treatment recommendations. They may nod in the room but ignore the advice at home. Conversely, when a strong bond exists, the patient becomes a partner in their recovery, motivated to do their homework because they understand the “why” behind the advice.
Techniques for Building Rapport Quickly
In a spa or clinic setting, you may not have a long history with the person on the table. You might need to establish rapport quickly. This requires efficiency of connection.
- Warmth in the First 10 Seconds: Smile and make eye contact immediately. The initial visual assessment determines safety.
- Use Their Name: People respond to the sound of their own name. It personalizes the interaction instantly.
- Physical Confidence: Touch with certainty. Tentative touch induces anxiety. Firm, respectful contact signals competence.
These small adjustments bridge the gap between strangers and partners in minutes. Consciously building these habits is essential for success.
Navigating Difficult Client Connections
Not every personality meshes instantly. You will encounter individuals who are guarded or skeptical. We view difficult client connections as opportunities to refine skills.
When resistance arises, do not take it personally. Often, a difficult demeanor masks pain. By remaining calm and consistent, you provide a stable anchor. We use “mirroring” techniques—matching the volume and pace of the speaker—to de-escalate tension. If rapport cannot be established, it is ethical to refer them to a different provider. Recognizing this is a sign of a mature therapist.
The RSM Approach to Holistic Training
At RSM International Academy, we do not view the physical and the psychological as separate. A tight hamstring is often connected to a guarded nervous system. Treating one without acknowledging the other is incomplete.
We train our students to be complete practitioners. They understand that your clients are looking for relief, and that relief comes from a combination of skilled touch and felt safety. We must honor their willingness to be vulnerable. Every gesture should reinforce safety, from the way we leave the room to allow them to undress, to how we manage comfort communication.
The Long-Term Value of Relationships
A successful career is built on retention. It is far more difficult to constantly recruit new people than it is to maintain existing relationships. By focusing on rapport, you build a loyal base. These individuals become advocates, referring friends because they trust your character as much as your hands.
Success in this field requires a synthesis of art and science. By prioritizing rapport, you elevate your massage therapy practice beyond simple mechanics. You create a space where recovery is optimized. This is the standard we set at RSM: developing therapists who are as empathetic as they are educated. By looking at the person, not just the muscle, you will find that your results improve and your work becomes deeply rewarding.
