
RSM Blog: Manual Therapy Techniques
Advanced Orthopedic Massage Techniques in Modern Therapy

Advanced orthopedic massage techniques
Clinical Precision in Bodywork
In my years of clinical practice I have often observed practitioners treating symptoms rather than systems. They rub the area that hurts. However, pain is rarely a local event; it is the final signal in a chain of biomechanical failures. This distinction drives our Orthopedic Massage Course. We do not just teach students to rub tissues; we teach them to act as clinical investigators.
Defining Orthopedic Massage in Practice
Orthopedic massage is not a singular modality but a comprehensive system of assessment and treatment. It focuses on correcting soft tissue conditions and structural dysfunctions that restrict function. Unlike a standard spa session, where the goal is sedation, this approach utilizes a multidisciplinary framework. It integrates anatomy and biomechanics to restore balance.
When a client presents with a complaint, the massage is secondary to the assessment. For example, if the gluteus medius is inhibited, the Tensor Fasciae Latae (TFL) often compensates, creating lateral knee pain. A therapist who only rubs the knee will fail. The therapy must address the inhibited gluteal muscle and the hypertonic TFL to resolve the issue permanently.
This clinical precision is what separates a relaxation provider from a highly skilled massage therapist. We focus on the restoration of capability. By manipulating the structures that surround the skeletal frame, we can alleviate chronic holding patterns that lead to pathology.
Core Massage Techniques for Restoration
To achieve these structural changes, we employ specific manual interventions. These massage techniques address specific physiological layers, ranging from breaking down adhesions to resetting neuromuscular tone.
We utilize the following approaches:
- Deep Tissue Massage: True deep tissue massage involves sinking through the superficial fascia to access sub-layer musculature. We teach students to melt through layers, engaging the structure without forcing it.
- Tissue Mobilization: This involves scooping and shearing forces to separate stuck tissue layers. Effective tissue mobilization restores the ability of individual muscles to slide past one another.
- Muscle Energy Techniques (MET): Using active contraction against resistance to lengthen shortened tissues without aggressive stretching.
These tools allow the therapist to remodel tissue. This is particularly relevant for sports injuries orthopedic specialists diagnose, such as tendonitis. We physically alter the structural composition of the tendon to encourage healing.
Restoring Mobility Through Joint Action
Soft tissue work alone is sometimes insufficient. The relationship between the contractile unit and the joint is symbiotic. Therefore, orthopedic massage must address joint mechanics.
At RSM, we emphasize joint mobilization. This is not chiropractic adjustment, but the gentle oscillation of articular surfaces. For instance, “frozen shoulder” involves a restriction in the joint capsule. While working on the rotator cuff is helpful, it does not address the capsular restriction. By integrating gentle joint mobility work, we create the space for mechanics to normalize.
This integration defines the advanced therapy we practice. It signals to the nervous system that the range of motion is safe, allowing the brain to reduce protective guarding.
Case Studies: Treating the Lower Back
Low back pain is perhaps the most common complaint we encounter. In many cases, the Quadratus Lumborum (QL) is blamed. However, treating the QL is often treating the victim, not the criminal.
The QL often becomes hypertonic because the Gluteus Medius is weak. If the glute fails to stabilize the pelvis, the QL works overtime. Digging an elbow into the QL offers only temporary relief. The treatment must involve releasing the QL followed immediately by activation work for the glutes.
Another culprit is the Psoas Major. A tight Psoas pulls the spine into hyper-lordosis, compressing the lumbar region. Here, the therapy involves deep abdominal work. The relief is often instantaneous as the lumbar curve settles into alignment.
The RSM Approach to Treatment
At RSM, we train students to see the body as a tensegrity structure. When one strut fails, the network shifts. Orthopedic massage is the science of identifying that primary failure.
Our approach bridges the gap between manual therapy and rehabilitation. We often recommend corrective exercises to support the manual work, ensuring patients do not become dependent on the therapist. Whether treating athletes or clients recovering from surgery, the goal is autonomy.
Musculoskeletal issues evolve based on how the body is used. Consequently, the treatment plan must adapt. Many styles of massage orthopedic practitioners favor focus on symptoms; we focus on solutions. By mastering these orthopedic techniques, therapists position themselves as essential healthcare providers. This is the standard we uphold at RSM.
The Science of Improving Mobility with Myofascial Release
Dynamic Myofascial Release Course
At RSM International Academy, we frequently encounter students and clients who confuse flexibility with mobility. They assume that an inability to touch their toes indicates short hamstrings, leading them to stretch aggressively. Yet, the stiffness often remains. This stagnation usually stems from a misunderstanding of the body’s architecture. The limitation is rarely a lack of muscular length; it is often a loss of sliding potential within the fascial tissues.
My approach, grounded in my background as an MSc in Sports Medicine, focuses on the causal chains that restrict movement. True mobility requires the independent gliding of muscles, nerves, and vascular structures. When these structures adhere due to trauma or overuse, standard stretching is ineffective. Instead, as we teach in our Dynamic Myofascial Release Course, we must focus on increasing mobility by addressing the connective architecture directly.
Understanding Myofascial Release Mechanisms
To understand why mobility is lost, we must look at the fascial tissues. Fascia is a continuous, three-dimensional matrix lubricating every muscle and organ with Hyaluronan. Under normal conditions, layers slide effortlessly. However, mechanical stress transforms this lubricant into a glue-like substance, a process known as densification.
This adhesion creates a mechanical barrier. When a patient attempts to move, the internal structures cannot slide. The brain perceives this resistance and inhibits muscle activation. Myofascial release works by applying sustained shear force to these densified areas. The friction reduces the viscosity of the hyaluronan, restoring the gliding potential of the soft tissue. Once the layers separate, the range of motion improves immediately.
Addressing Chronic Muscle Tension
It is critical to distinguish between neurological tightness and mechanical restriction. In our clinic, we see many clients with chronic “tight shoulders” who find no lasting relief from standard massage. They treat the symptom—the tension—without addressing the container—the fascia.
Muscle tension is often a protective response. When the fascial envelope becomes rigid, it acts like a shirt that is two sizes too small. The muscle fibers inside are compressed, leading to ischemia (lack of blood flow). This oxygen deprivation causes the muscle to contract further, creating a cycle of pain. Standard massage presses the muscle against the bone, which fails to expand the “shirt.” In contrast, manual therapy aiming for structural integration elongates the fascial planes. By expanding the container, we remove the mechanical compression, and the pain signals dissipate.
The Role of Trigger Points
Mobility is also compromised by trigger points—specific physiological lesions within skeletal muscle. A trigger point forms when a metabolic crisis locks actin and myosin filaments into a continuous contraction. This cuts off local oxygen supply, creating an acidic environment that sensitizes pain receptors.
A trigger point in the hip, for example, can mimic sciatica. In our therapy courses, we teach students to use ischemic compression to treat these spots. By temporarily blocking and then releasing blood flow, we flush the tissue with oxygen, breaking the metabolic crisis. This restores the muscle’s ability to lengthen, thereby improving mobility with myofascial release.
Self-Myofascial Release vs. Manual Therapy
The fitness industry has popularized self-myofascial release using foam rollers. While myofascial rolling is valuable for warming up or resetting neural tone, it has limitations. A foam roller applies broad compression; it cannot distinguish between nerve entrapment and fascial adhesion.
Mechanical restrictions often require a specific vector—a direction of pull—to release. A skilled therapist uses their hands to hook into the body and apply precise shear force. Furthermore, rolling requires active muscle contraction to stabilize the body, whereas manual therapy allows the patient to remain passive. This passivity grants the therapist access to deeper myofascial layers that are inaccessible when muscles are engaged.
Restoring Functional Capacity
The ultimate goal of any therapy at RSM is not just temporary pain relief, but the restoration of function. Pain is merely the signal; dysfunction is the problem.
Consider a runner with lower back pain. The cause is often adhered hip flexors preventing hip extension. This forces the lumbar spine to over-extend to compensate. Treating the back offers only temporary relief. The solution requires a targeted fascia release of the Psoas. By freeing the hip, we spare the spine.
At RSM, we teach release techniques that respect the thixotropic nature of fascia. We do not force the tissue; we sink and wait for the body to yield. This approach ensures that we are not just relaxing the patient, but permanently improving their biomechanics. Through the intelligent application of myofascial release, we provide a pathway to a mobile, functional, and pain-free life.
Pelvic Rotation Patterns and Their Impact on the Piriformis and Sciatic Nerve in Right-Dominant Athletes

Athletes who rely heavily on their right side, such as right-handed golfers, tennis players, and rotational-sport practitioners, often develop a predictable pattern of muscular tension around the pelvis and posterior hip. These adaptations are not random; they arise from repeated movement strategies that place asymmetrical forces on the deep hip rotators, the piriformis muscle, and the neural structures that pass beneath or through it. In many right-dominant athletes, the pelvis tends to rotate toward the left during the swing or stroke phase, creating increased demand on the right posterior chain while the left side becomes the anchor for stability and directional control.
From a muscular perspective, the right piriformis and the lateral portion of the right hamstring frequently become overactive because they must decelerate the rapid left-rotational motion of the pelvis. Over time, this load may produce stiffness or localized tenderness in the deep gluteal region. On the opposite side, the left hip commonly demonstrates increased tension in the tensor fasciae latae, the gluteus medius and minimus, the adductor group, and the medial hamstrings. These muscles function as stabilizers during rotation and often accumulate tension as they control the rotational axis of the pelvis.
This pattern is clinically relevant because approximately ten to seventeen percent of the general population exhibits anatomical variations in the relationship between the piriformis and the sciatic nerve. In some individuals, part of the sciatic nerve may pass above, below, or even through the piriformis. When this variation is combined with rotational sports, the likelihood of compression or irritation increases, especially as athletes reach their mid-thirties and forties. Reduced muscle elasticity, mild fibrosis in the deep hip rotators, and decreased neural glide contribute to symptoms such as buttock pain, posterior thigh discomfort, or sensitivity along the ischial region.
Assessment should begin with a structured sequence. The FAIR position—hip flexion, adduction, and internal rotation—remains one of the most practical ways to engage the piriformis and observe irritation patterns. Maintaining the hip near sixty degrees of elevation is essential, as this angle maximally loads the deep external rotators. The location of the athlete’s pain provides useful diagnostic clues. Deep pain near the ischium or the lateral hamstring region may suggest involvement of the inferior cluneal nerve. Medial hamstring discomfort or symptoms closer to the inner thigh more commonly point to tension in the posterior femoral cutaneous nerve. If the athlete reports isolated deep-gluteal pressure, a pure piriformis tightness pattern is likely.
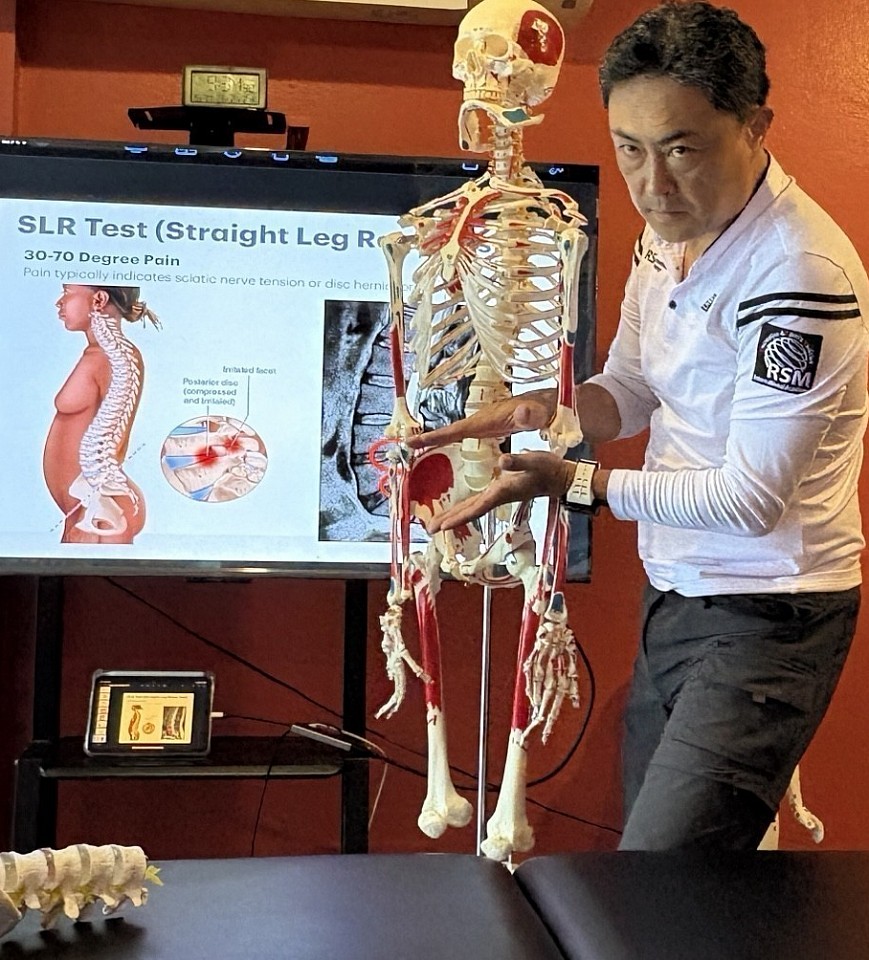
A second stage involves assessing neural mobility. Extending the knee from the testing position increases tension along the tibial nerve and the deep fibular nerve. Restrictions here may recreate symptoms along the calf or even near the peroneus longus, indicating reduced neural glide rather than a muscular source of pain. The Straight Leg Raise and its variations help determine whether the problem originates from the nerve or from the surrounding soft tissue.
If symptoms improve with myofascial release, trigger point therapy, or neural-glide techniques, the primary issue is usually functional. However, persistent symptoms despite appropriate manual therapy may indicate an underlying structural factor, such as an anatomical variation of the sciatic nerve or true deep-gluteal entrapment. In those cases, referral to a physician is appropriate. Ultrasound-guided injections—performed with imaging rather than a blind approach—are now the clinical standard when conservative care is insufficient. They offer both diagnostic clarity and therapeutic value without the risks associated with unguided injections into the deep hip.
This integrative approach, combining movement analysis, soft-tissue assessment, and neural evaluation, provides a reliable framework for understanding and treating posterior hip pain in right-dominant rotational athletes. It respects both the complexity of pelvic mechanics and the individual variations that influence symptoms, allowing clinicians and practitioners to guide athletes toward safer and more efficient movement patterns.
- Hironori Ikeda, MSc Sports Medicine
Neurodynamics & Sports Biomechanics Specialist
References
1 ) Beaton, L. E., & Anson, B. J. (1937). The relation of the sciatic nerve and its subdivisions to the piriformis muscle. Anatomical Records.
2)Windisch, G., Braun, E. M., Anderhuber, F., & Ulz, H. (2007). Anatomical variations of the piriformis muscle and the sciatic nerve. Clinical Anatomy.
Safe Manual Therapy Strategies for Lumbar Spondylolisthesis and Extension-Related Symptoms
Lumbar Lordosis and Pelvic Anterior Tilt
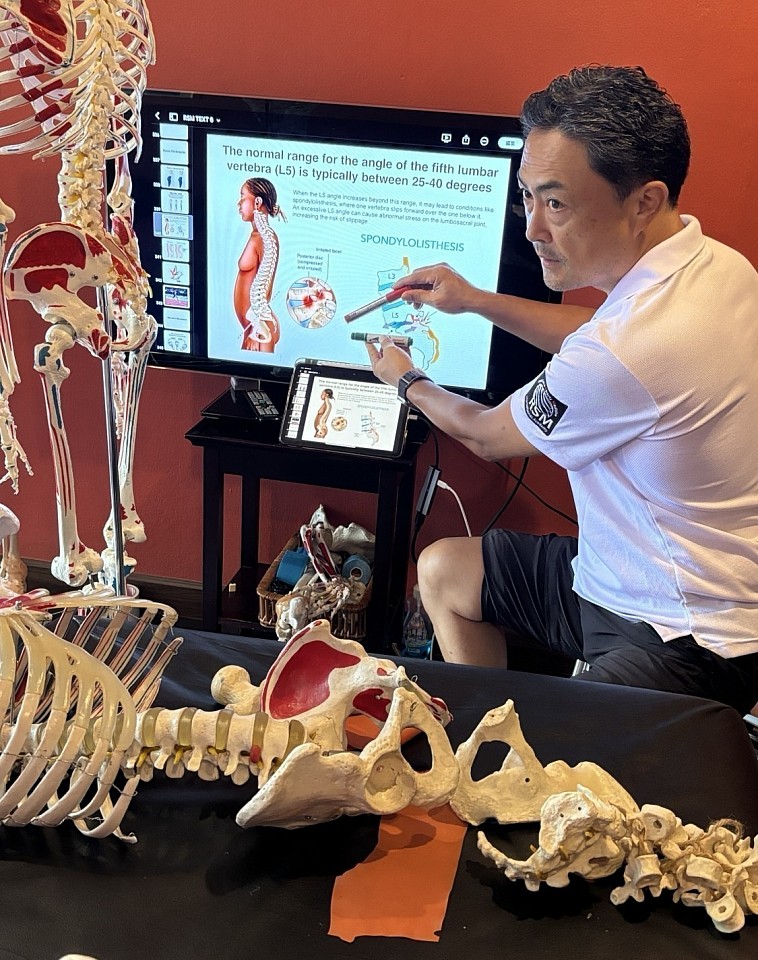
Lumbar spondylolisthesis is one of the conditions where symptoms often intensify during extension. Athletes and trainers who spent their younger years lifting heavy weights, teaching weight training, or loading the lumbar spine repeatedly frequently present with this pattern. Many of them felt “strong” in their twenties and thirties, yet early signs of instability were already present. When these individuals reach their mid-fifties and begin to gain weight, the unstable motion segment becomes symptomatic and the condition progresses into a clear spondylolisthesis. I have seen this repeatedly in the last three to four years, particularly among former weightlifting instructors who can no longer perform or teach lifts and now depend on developing manual therapy skills to maintain their careers.
In extension-sensitive spondylolisthesis, the forward slip of the vertebral body increases shear forces at the affected level, most commonly L4–L5 or L5–S1. Even a slight increase in lordosis can provoke burning, radiating discomfort, a sense of pressure across the lumbosacral junction, or irritation that spreads into the gluteal region or the leg. These patients often arrive already guarded, and even minor movements toward extension reproduce their pain.
For this group, positioning is the first treatment. A pillow placed under the chest increases lordosis and almost always worsens symptoms. A pillow placed under the abdomen does the opposite. It draws the lumbar spine toward a neutral or slightly flexed alignment and reduces anterior shear at the slipped segment. When both knees are gently brought toward the chest and traction is applied slowly, many patients experience immediate relief, not because of force but because the canal opens just enough to calm the irritated nerve root.
Manual therapy must respect the mechanical instability. Deep tissue pressure directly over the lumbar facets or into the multifidus is rarely beneficial at this stage and may trigger further muscle guarding. Selective work is more effective. Trigger point techniques can be applied safely to symptomatic myofascial regions around the lumbar spine, gluteal complex, and lateral hip without loading the unstable level itself. Controlled manual contact reduces peripheral tension while protecting the deeper stabilizers that the patient still depends upon.
Understanding the segmental level matters. In the clinical example, the narrowing and the forward slip are most consistent with L4–L5, although individual anatomy may differ. Regardless of the exact level, the principle remains constant. Flexion bias reduces symptoms, while extension increases neural irritation and should be avoided in early stages.
What has become increasingly clear in my own clinical work is how often former trainers follow this pattern. Many of them lifted heavy loads for decades, then slowed down, gained weight, and now find themselves unable to demonstrate or teach weightlifting technique. They turn toward massage therapy and clinical bodywork because it becomes their livelihood. These therapists must not only protect their own spine but must also recognize the same risk factors in their clients. Spondylolisthesis is not rare among former strength athletes, and understanding safe manual strategies is part of professional survival.
A careful combination of flexion-biased positioning, symptom-controlled manual therapy, and precise palpation offers a practical and safe method for managing this condition. When symptoms become stable, gradual strengthening and controlled movement retraining can begin. The priority in early care is always protection of the unstable segment and avoidance of strategies that increase extension stress.
This is not theory. It is a pattern I have observed repeatedly across many years of working in sports medicine. The athletes and trainers who developed spinal instability early in life and gained weight later often present with the most predictable extension-aggravated symptoms. Their clinical presentation, response to manual therapy, and recovery pattern follow the same logic. My goal is to offer a framework that therapists with one or two years of experience can apply safely, while still reflecting what senior clinicians encounter in practice.
- Hironori Ikeda, MSc Sports Medicine
Neurodynamics & Sports Biomechanics Specialist
References
1) Kalichman, L., & Hunter, D. (2008). Lumbar spondylolisthesis: A systematic review of the literature. Spine Journal.
2) Murtagh, R. (2008). Diagnosis and conservative management of spondylolisthesis. American Journal of Physical Medicine & Rehabilitation.
Sports Medicine Approach to Upper-Extremity Pain and Kinetic-Chain Dysfunction
Thoracic outlet syndrome
Upper-extremity disorders such as Pronator Teres Syndrome, Carpal Tunnel Syndrome, and De Quervain’s tenosynovitis cannot be understood in isolation. In sports medicine, these conditions emerge from failures across the kinetic chain: shoulder rotation, forearm pronation mechanics, wrist deviation control, tendon glide, neural tension, and joint centralization. When even one link in this chain loses mobility or alignment, the athlete compensates, and the overload expresses itself where the system is weakest.
In advanced assessment, we look first at the essential movement triad: glenohumeral internal rotation, forearm pronation, and wrist flexion–ulnar deviation coupling. These motions must work together in a synchronized pattern for throwing, tennis strokes, golf swings, and high-velocity upper-limb actions. When GH internal rotation is restricted, the athlete is forced to overuse the forearm, especially the pronator teres. When wrist mobility—particularly flexion and ulnar deviation—is limited, the body generates power through compensatory forearm pronation rather than through the shoulder–trunk system. Over time, this creates fibrosis, altered tendon glide, neural tension, and joint malalignment that eventually present as pain.
Joint centralization plays a critical role in performance and injury prevention. When the glenohumeral joint, elbow joint, radiocarpal joint, or thumb CMC joint falls outside its ideal position, the surrounding tissues must absorb abnormal load. Without centralization, the kinetic chain cannot transfer energy efficiently, and the body responds with compensatory recruitment patterns. These are the patterns we routinely identify at RSM International Academy during our Sports Medicine Massage and Trigger Point Therapy training.
In de Quervain’s tenosynovitis, loss of glide in the first dorsal compartment prevents the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) from moving smoothly beneath the extensor retinaculum. The tendon sheath thickens, the retinaculum becomes less compliant, and the thumb CMC joint often shifts slightly from its centered position. This misalignment increases friction, amplifies mechanical stress, and produces the classic radial-sided wrist pain commonly seen in massage therapists, caregivers, and female practitioners in their forties and fifties. In many of these cases, the problem is not inflammation—it is a failure of myofascial glide, tendon glide, and joint centralization.
In my clinical experience, a targeted five-to-eight-minute intervention—restoring retinacular mobility, improving sheath elasticity, releasing APL/EPB adhesions with cross-fiber techniques, and applying precise high-velocity low-amplitude mobilization to the thumb CMC joint when indicated—can dramatically reduce pain. This rapid response demonstrates the mechanical nature of the dysfunction and the importance of restoring glide and centralization.
Pronator Teres Syndrome follows a similar logic. When GH internal rotation is limited or the athlete over-relies on forearm pronation to generate power, the pronator teres becomes chronically overloaded. Fibrosis forms between its two heads, and the median nerve loses its ability to glide. Neural tension increases, forearm mechanics collapse, and wrist-control muscles overwork to compensate. At RSM International Academy, therapists learn the Pronator Teres Provocative Test, which uses resisted pronation with varying elbow flexion to identify nerve compression at the pronator. This differentiates it from distal compression inside the carpal tunnel, allowing precise treatment rather than generalized forearm work.
Accurate assessment is central to RSM’s methodology. The Finkelstein test remains the most reliable provocation method for de Quervain’s, while the Pronator Teres Provocative Test isolates proximal median nerve compression. But evaluation never stops at the pain site. Students are trained to examine GH internal rotation, scapular rhythm, neural glide throughout the brachial plexus, wrist flexion–ulnar deviation coupling, and thumb CMC joint alignment. Only by connecting these elements can a therapist identify true causation rather than chasing superficial symptoms.
Treatment at RSM International Academy integrates Trigger Point Therapy, Sports Medicine Massage, joint mobilization (HVLA/LVLA), myofascial release, and neural mobilization into a single unified system. Trigger points in the pronator teres, flexor carpi radialis, brachioradialis, and intrinsic thumb muscles are released not as isolated techniques but in coordination with joint corrections and nerve-glide restoration. Our approach views pain as the final output of a dysfunctional kinetic chain, not the primary target.
Athletes who fail to maintain centralization and aligned movement patterns eventually overload the wrist and thumb structures. When the wrist lacks mobility—especially flexion or ulnar deviation—the body compensates with excessive pronation during strokes or swings. This compensation loads the pronator teres, tightens the APL and EPB, increases retinacular stress, and ultimately produces nerve and tendon pathology. Correcting these movement faults restores efficient load distribution and allows athletes to perform with power, speed, and longevity.
RSM’s training is fundamentally about teaching therapists to see this big picture. By combining sports medicine principles with hands-on manual therapy, our programs prepare practitioners to identify the true source of dysfunction, restore alignment and glide across all tissues, and deliver results that matter in real-world human movement.
Disclaimer: This article is for educational purposes only. Persistent numbness, weakness, or night pain should be evaluated by a medical professional.
- Hironori Ikeda, MSc sports medicine
Neurodynamics & Sports Biomechanics Specialist
Eeference
1) Goel R, Abzug JM. De Quervain’s Tenosynovitis: A Review of the Rehabilitative Options. Hand (N Y). 2015 Mar;10(1):1–6. doi:10.1007/s11552-014-9652-7.
2) Sharma K, Dididze M, Ganesh A. Pronator Teres Syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526090/
Sports Massage Assessment Techniques: Mastering Clinical Precision

Sports massage course students at RSM International Academy
In manual therapy, technical skill in delivering strokes is only half of the equation; true clinical effectiveness comes from structured assessment grounded in biomechanics, functional anatomy, and the behavior of the kinetic chain. At RSM International Academy, practitioners in our Sports Massage Course learn that moving beyond a basic intake form into orthopedic-grade evaluation elevates the precision of their therapy.
While research on manual therapy’s influence on kinetic-chain mechanics is still developing, clinical practice and movement analysis consistently indicate that understanding joint mechanics and tissue responsiveness before treatment improves the relevance and accuracy of manual interventions. This evidence-informed approach establishes a professional standard where each session is intentional, targeted, and aligned with the client’s specific performance demands.
Subjective Evaluation: The Interview
The assessment begins with the investigative phase. While beginners may simply ask, “Where does it hurt?”, the intermediate therapist uses structured questioning to understand the mechanism of injury. Is the condition acute, sub-acute, or chronic? This classification controls treatment intensity; for example, deep friction is contraindicated in the acute inflammatory phase. To accurately profile pain, therapists apply the OPQRST framework (Onset, Provocation, Quality, Region, Severity, Timing).
At RSM International Academy, this process also includes identifying pain-avoidance posture and antalgic lean, recognizing how clients unconsciously change alignment to escape pain. This helps determine which movements in the kinetic chain trigger symptoms and which joints are absorbing excess load. By integrating these observations, the interview becomes more than a checklist—it becomes a clinically meaningful analysis that guides precise and targeted manual therapy.Objective and Visual Analysis
Once the history is taken, we move to objective observation using the “Plumb Line” approach. Visual analysis identifies kinetic chain imbalances that contribute to dysfunction.
- Anterior View: Check for knee valgus or leg length discrepancies.
- Lateral View: Crucial for spinal evaluation. Look for Forward Head Posture (FHP) or Anterior Pelvic Tilt, which dictates whether you need to lengthen hip flexors or hamstrings.
- Posterior View: Observe scapular positioning and Achilles tendon alignment.
Functional Evaluation: Range of Motion (ROM)
Static posture gives us a map, but the body is designed for movement. Functional assessment tests the integrity of specific tissues:
- Active ROM (AROM): The client moves the joint unassisted. Pain here indicates muscle strain or joint issues.
- Passive ROM (PROM): The therapist moves the relaxed limb. If AROM is painful but PROM is pain-free, the issue is likely muscular (contractile tissue). If PROM is also painful, the issue may be articular (ligament/capsule).
- Resisted ROM (RROM): Testing isometric strength to identify lesions in the muscle-tendon unit.
Palpation and Special Tests
While visual and functional tests provide data, palpation is where the massage therapist truly shines. Clinical palpation requires differentiating tissue states—distinguishing between hypertonicity (tight muscle), fibrosis (scar tissue), and edema (swelling).
To truly specialize in sports care, you must also be familiar with “Special Tests.” These provocative maneuvers stress specific structures to identify pathology. Examples include:
- The Empty Can Test: Assesses the Supraspinatus tendon for rotator cuff tears.
- The Thomas Test: Differentiates tightness between the Iliopsoas, Rectus Femoris, and TFL.
- Ober’s Test: Identifies tightness in the IT Band, crucial for runners with knee pain.
Mastering Sports Massage Improves Performance and Recovery
Advanced sports massage evaluation techniques allow you to navigate complex musculoskeletal issues with confidence. By linking assessment data directly to your treatment plan, such as releasing a fibrotic TFL to cure lateral knee pain, you ensure that your therapy is purposeful and effective.
For the therapist, the journey involves moving beyond intuition and embracing a systematic, evidence-based approach. By integrating detailed history taking, functional ROM testing, and specific orthopedic evaluations, you provide a higher standard of care that leads to faster recovery and better performance outcomes for your clients.
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
Reference
1) HL Davis et al. (2020). Effect of sports massage on performance and recovery. PMC.
2) B Liza et al. (2023). Effectiveness of manipulative massage therapy in pain, ROM and shoulder function (pdf).
Sports Medicine Massage Course in Chiang Mai
The Difference Between Sports and Deep Tissue Massage
For individuals dealing with chronic pain, limited mobility, reduced flexibility, or a limited range of motion, the terminology used in rehabilitation and wellness can easily become confusing. Two treatments that often seem similar on the surface are sports massage and deep tissue massage, mainly because both aim to relieve physical discomfort. In reality, their purposes and physiological focus are very different. Deep tissue massage addresses postural deviation, chronic holding patterns, and deeper layers of muscle and connective tissue—work that improves movement quality and long-term structural alignment. Sports massage, on the other hand, is closely connected to sports conditioning management, performance readiness, and maintaining optimized movement for active individuals.
At RSM International Academy, our Sports Massage Course emphasizes understanding when and why each modality should be applied. Using deep tissue techniques to correct alignment and resolve adhesions is not the same as using sports massage to support recovery, manage training load, or maintain functional biomechanics. Whether you are a client seeking treatment or a therapist in training, recognizing this distinction leads to more accurate injury management and more consistent improvements in optimized movement and overall body mechanics.
What is Deep Tissue Massage?
Deep tissue massage is a structural integration approach, and in the RSM method it is also used to restore joint centralization and improve kinetic chain alignment. Although it is often mistaken for “a very hard massage,” true deep tissue work depends on precision, myofascial layering, and understanding how deeper structures influence posture and movement, not on force. The goal is to resolve chronic strain, postural deviation, and misalignment within the kinetic chain by targeting the deeper layers of muscle and connective tissue while enhancing overall movement quality.
During our Deep Tissue Massage Course the therapist uses slow, deliberate strokes to move from the superficial into the deep myofascial layers, focusing on muscle glide, intermuscular mobility, and tension patterns without provoking protective tightening. Sustained pressure with knuckles, elbows, and forearms helps break down adhesions and scar tissue, while equal emphasis is placed on therapist positioning, the direction of applied pressure, and the mechanics required to reach deeper structures. In the RSM system, deep tissue work not only releases chronic holding patterns—such as a stiff neck, low-back tightness, or forward head posture—but also improves joint centralization and optimizes kinetic chain alignment, leading to more efficient and pain-free movement.
What is Sports Massage?
The RSM Sports Massage Course teaches a targeted and dynamic method rooted in biomechanics and sports-related injuries, designed for anyone who places continuous physical stress on the body. This approach emphasizes sports conditioning management, focusing on maintaining joint mobility, tissue elasticity, and proper kinetic-chain alignment throughout training cycles. Techniques adapt to purpose—pre-event work activates the neuromuscular system, post-event work clears metabolic waste, and maintenance work preserves movement efficiency and performance.
A key element of the RSM method is the integration of active components, including stretching, joint mobilization, and muscle-energy techniques. These tools are applied to improve kinetic-chain function, support joint-mechanics centralization, restore tissue elasticity, and keep the body performing efficiently under physical demand. The goal is not simply relaxation, but maintaining the body as a functional system capable of consistent performance.
Key Differences in Intent and Massage Techniques
The divergence between the two lies in the intent of the session.
- Speed and Rhythm: Deep tissue is slow. To sink into the deep layers of the body, the therapist must wait for the tissue to melt. Sports massage varies in tempo and is often brisk to stimulate blood flow and nervous system response.
- The Focus: Deep tissue is problem-oriented regarding chronic pain and structure. It asks, "How does your posture affect your pain?" Sports massage is outcome-oriented. It asks, "How does this muscle tension affect your running stride or your squat?"
- Passive vs. Active: In deep tissue, the client is usually passive. In sports massage, the client is often active, moving limbs against resistance to engage the nervous system.
Which Do You Need: Sports Massage or Deep Tissue Massage?
If your goal is to fix long-term postural issues, relieve chronic back pain from sitting, or break up old scar tissue, deep tissue massage is the correct choice. It releases the tension that pulls the body out of alignment.
If your goal is to recover from a workout, improve your flexibility for a specific sport, or prevent injury during training, sports massage is the superior option. It focuses on keeping the soft tissues elastic and responsive.
The RSM Approach for Aspiring Massage Therapists
Ultimately, the most effective treatment often requires a blend of both. A massage therapist trained at RSM International Academy learns to integrate these styles based on clinical assessment. We teach our students that you cannot effectively perform either modality without a profound understanding of functional anatomy and clinical palpation. By bridging the gap between these techniques using sports medicine principles, we ensure that every massage is a step toward better health, posture, and performance.
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
References
1) Dakić, M., Toskić, L., Ilić, V., Durić, S., Dopsaj, M., & Šimenko, V. (2023). The Effects of Massage Therapy on Sport and Exercise Performance: A Systematic Review. Sports (Basel). [PMC]
2) Jones, T. A. (2004). Rolfing, or Structural Integration: A Review of the Evidence. Journal of Bodywork & Movement Therapies. [PubMed]
Cluneal Neuralgia or Piriformis Syndrome? How to Differentiate SI Joint Pain, Deep Gluteal Syndrome and Sciatica

Deep tissue massage for piriformis syndrome
In clinical sports medicine, not all buttock pain is sciatica. A relatively overlooked cause is cluneal neuralgia, particularly entrapment of the middle cluneal nerve beneath or through the long posterior sacroiliac ligament (LPSL). This often produces a superficial burning or stabbing sensation around the posterior iliac crest and upper buttock, closely resembling sacroiliac joint dysfunction or lumbar radiculopathy but not following a typical dermatomal distribution.
To distinguish cluneal neuralgia from piriformis syndrome and deep gluteal syndrome, I first differentiate between superficial cutaneous pain and deep myoneural pain. Palpation along the PSIS and the LPSL often reproduces symptoms associated with middle cluneal nerve entrapment. In contrast, deep pressure at the greater sciatic notch and along the short external rotators evokes a deeper stretching or radiating pattern consistent with sciatic or posterior femoral cutaneous nerve involvement. The FABER (Patrick) test helps determine whether the sacroiliac joint itself is the primary pain generator or if symptoms stem from periarticular ligament or nerve irritation.
Anatomically, the superior gluteal nerve and vessels pass above the piriformis through the suprapiriform foramen, while the sciatic nerve, inferior gluteal nerve and posterior femoral cutaneous nerve pass below it through the infrapiriform foramen. Variations in the course of the sciatic or posterior femoral cutaneous nerve, such as splitting or piercing the piriformis, explain why some athletes present with atypical deep gluteal pain that does not follow standard textbook patterns. Palpation landmarks such as the PSIS–greater trochanter line and the greater sciatic notch are useful, but it is important not to mistake the overlapping upper fibers of gluteus maximus and gluteus medius for the piriformis itself.
Once the primary pain source is identified, treatment becomes more precise. For cluneal neuralgia, the focus is on accurate palpation of the LPSL, releasing superficial fascial restrictions and reducing irritation around the nerve pathway. For piriformis syndrome and deep gluteal syndrome, cross-fiber soft-tissue mobilization, active mobilization of the piriformis and the deep external rotators and nerve-gliding techniques for the sciatic and posterior femoral cutaneous nerves help restore mobility in the greater sciatic notch region. This anatomical and layer-specific approach consistently produces better outcomes than generalized deep tissue massage.
If you want to study the palpation skills, pain differentiation, and clinical treatment strategies in greater depth, you can learn them in our Trigger Point Therapy and Deep Tissue Massage programs at RSM International Academy.
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
References
1)Anderson D. A comprehensive review of cluneal neuralgia as a cause of low back pain. 2022.
2)Martin HD, Reddy M, Gómez-Hoyos J. Deep Gluteal Syndrome: anatomy, imaging, and management of sciatic nerve entrapments in the subgluteal space. 2015.

Trigger point therapy around superior cluneal nerve,
Heel-Strike Dominance, Tightness in the Posterior Gluteal Fibers, and the Role of the Superior Cluneal Nerve
Clients who land heavily on their heels often present with clear tightness in the posterior fibers of the gluteus medius and the upper fibers of the gluteus maximus. Therapists encounter this pattern repeatedly, especially in individuals whose pelvic control relies heavily on these muscles to absorb the shock generated at heel strike. As these muscles tense over time, fascial glide decreases, creating persistent stiffness and trigger points around the upper and lateral gluteal region.
An important but frequently overlooked factor in this pattern is the Superior Cluneal Nerve. Originating from the dorsal rami of L1 to L3, the nerve passes through the thoracolumbar fascia, crosses the quadratus lumborum and multifidus, and travels over the iliac crest near the PSIS before entering the upper gluteal area. This region along the iliac crest is particularly prone to entrapment. When the nerve becomes restricted, discomfort and radiating tension across the upper gluteal region can worsen, especially when the surrounding musculature is already overworked.
People who show mild Trendelenburg-type pelvic drop during gait often display not only muscle tension but also decreased neural mobility in this area. This makes the pelvis less stable with each step, not simply because of muscle weakness, but due to a combination of neural entrapment and fascial tension around the posterior hip. Athletes who engage in running, golf, or rotational sports commonly develop this pattern.
At RSM International Academy, practitioners study these gluteal and neural interactions in detail through Trigger Point Therapy and Deep Tissue Massage. The approach includes deep release of the posterior gluteus medius, targeted treatment of upper gluteus maximus trigger points, and techniques aimed at restoring mobility around the superior cluneal nerve near the iliac crest. Improving the glide of the deep fascial layers in this region consistently helps reduce low-back discomfort and upper gluteal pain, making it a highly reliable treatment zone.
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
References
1) Maigne JY, Doursounian L. Entrapment neuropathy of the superior cluneal nerves. Spine. 1997;22(10):1156–1159.
2) Lu J, Ebraheim NA, Huntoon M, et al. Anatomic considerations of the superior cluneal nerve at the posterior iliac crest region. Clin Anat. 2000;13(3):139–143.
Kinetic Chain Dysfunction as the Hidden Driver of Forearm Pain

Kinetic Chain Dysfunction in Upper-Limb Pain
Forearm pain, especially Pronator Teres Syndrome and Carpal Tunnel Syndrome, is frequently misinterpreted as a localized forearm disorder. From a sports medicine perspective, however, these symptoms most often arise from disruptions within the kinetic chain linking the glenohumeral joint, the forearm, and the wrist. The essential biomechanics of the upper limb are organized into two primary movement pathways:
1. GH Internal Rotation → Forearm Pronation → Wrist Ulnar Deviation
2. GH External Rotation → Forearm Supination → Wrist Radial Deviation
When mobility restriction or neuromuscular dysfunction occurs at any point along these pathways, deep forearm muscles such as the pronator teres, flexor digitorum superficialis, and flexor digitorum profundus contract excessively as a compensatory strategy. This pattern significantly increases the likelihood of Median Nerve Glide Dysfunction, a mechanism consistently supported by sports medicine literature.
A particularly common clinical finding is reduced external rotation capacity of the rotator cuff, specifically the infraspinatus and teres minor. Movements that should be absorbed through GH external rotation are instead diverted into excessive forearm pronation, leading to chronic overactivation of the pronator teres and deep flexor group. This compensation pattern—GH ER restriction → increased forearm flexor tone → neural mobility impairment—is one of the most reproducible mechanisms observed across clinical practice.
This phenomenon is clearly visible in various sports settings.
Judo gripping actions require repeated traction and rotation with the wrist fixed, dramatically elevating pronation load. Martial arts impose continuous gripping and rotational acceleration, producing chronic fatigue in the deep flexor–pronator complex. Yoga handstands fix the wrist under load, increasing isometric tension in the forearm. Baseball pitching, the golf downswing, and tennis forehand strokes all involve pronounced pronation combined with ulnar deviation, making pronator teres stiffness highly prevalent among athletes.
The common denominator across these activities is that the wrist remains mechanically locked while compensatory load concentrates in the forearm, leading to progressive myofascial adhesions and deterioration of median nerve mobility. Localized treatment alone rarely produces lasting improvement because it overlooks the integrated nature of the upper-limb kinetic chain.
At RSM International Academy, directed by Hironori Ikeda, clinical assessment centers on the shoulder–forearm–wrist kinetic chain. The academy emphasizes comprehensive evaluation of GH external rotation restriction, scapular motion control, restoration of median nerve mobility through nerve-glide techniques, dynamic myofascial release of deep fascial structures, and high-level palpation skills indispensable for differentiating fiber orientation, fascial density, and neural pathways. Palpation training is directly integrated with functional anatomy to enable precise identification of the pronator teres, FDS, and FDP complexes.
When GH external rotation improves, compensatory forearm activation naturally diminishes, reducing hypertonicity even during tasks requiring wrist fixation. This represents the restoration of the authentic kinetic chain, producing stable and long-lasting clinical outcomes.
These concepts and techniques are systematically explored within the
1) Sports Massage Course,
2) Remedial Massage Course,
3) Dynamic Myofascial Release Course at RSM International Academy.
Each course is grounded in the sports medicine principle that the upper limb must be evaluated as a single functional movement system rather than isolated anatomical segments.
Ultimately, forearm pain, neural symptoms, and shoulder dysfunction may appear unrelated, yet when viewed through the kinetic chain, they align along a single continuum. A whole-chain perspective yields the most accurate, reproducible, and clinically valid approach in sports medicine.
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
References
1) Ludewig PM, Reynolds JF. The Association of Shoulder Dysfunction with Upper Extremity Nerve Entrapment Syndromes: A Kinematic Perspective. Journal of Orthopaedic & Sports Physical Therapy.
2) Werner SL, Fleisig GS, Dillman CJ, Andrews JR. Biomechanics of the Elbow and Forearm During Sports Activities. Clinical Sports Medicine.
Patellar Fat Pad Impingement and Kinetic Glide Chain Restoration: Clinical Approach to Chronic Anterior Knee Pain

Sports Medicine–Based Manual Therapy for Chronic Anterior Knee Pain
In clinical practice, anterior knee pain rarely stems from a single cause. When careful work on the patellar tendon or quadriceps tendon yields little improvement, the true source is often found behind the patella — within the infrapatellar fat pad (Hoffa’s fat pad).
This fat pad serves as a cushion for the knee, but when it becomes repeatedly compressed between the inferior pole of the patella and the anterior tibia, it can develop fibrosis and adhesions, leading to a condition known as Patellar Fat Pad Impingement. Chronic cases or post-meniscal injuries often present with this pattern, accompanied by a loss of superior–inferior patellar glide and deep anterior knee discomfort.
My initial clinical evaluation is straightforward yet highly informative. With the thumb stabilizing the inferior border of the patella and the index finger supporting the superior border, I gently mobilize the patella in all directions — superior, inferior, and circular motions — to assess tissue elasticity and fibrotic resistance.
When a “gritty” friction or marked discomfort is felt, I apply micro-mobilization combined with deep transverse friction while maintaining slight knee flexion (15–20°). The goal is to guide the fat pad posteriorly during flexion and allow smooth anterior glide during extension. As the tissue softens, patellar motion becomes smoother, and the patient often reports a clear release of the deep “pressure” sensation behind the knee.
A crucial element is correcting the lateral pulling tension that perpetuates this problem. In most cases of chronic patellar pain, excessive tension within the Tensor Fasciae Latae (TFL), Iliotibial Band (ITB), and Vastus Lateralis forms a dominant lateral kinetic chain that drags the patella laterally.
To release this, I first perform longitudinal fascial release along the Rectus Femoris–Vastus Intermedius interface, followed by cross-fiber release at the distal one-third. Next, I restore the mobility of the suprapatellar pouch through ASTR (Active Soft Tissue Release). Once these layers regain glide, patellar tracking improves and the kinetic glide chain reorganizes naturally.
At this point, I also check the function of the Popliteus muscle, which contributes to the screw-home mechanism of the knee. By gently activating this muscle in slight flexion, we can reestablish end-range rotational stability and centralize patellar tracking. Correcting the lateral drift not only reduces pain but also restores structural balance across the patellofemoral joint.
In many of my clinical cases, after about four to five sessions (roughly two weeks), patients show clear improvement: pain on stair climbing decreases from NPRS 6 to 2, and flexion-extension motion becomes smooth.
This is not simple “muscle loosening.” It represents the reconstruction of the kinetic glide chain among the quadriceps, patella, fat pad, and synovial membrane — an integrated dynamic system that governs patellofemoral tracking and deep knee mechanics. The infrapatellar fat pad is not just a soft cushion; it is a biomechanical regulator of anterior knee motion. Recognizing its role fundamentally changes how we treat chronic anterior knee pain.
At RSM International Academy, both the Deep Tissue Massage Course and the Remedial Massage Program systematically teach this biomechanical understanding of the patellar fat pad through a combination of structural assessment, mobilization, and fascial release.
Students don’t simply memorize techniques — they learn to determine which layer, in what order, and in which direction to mobilize. This logical, evidence-based reasoning is the essence of Sports Medicine–based Manual Therapy that RSM promotes worldwide.
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
References
1)Dye, S.F. (2005). The pathophysiology of patellofemoral pain: A tissue homeostasis perspective. Clinical Orthopaedics and Related Research, 436, 100–110.
2)Stecco, C., Gagey, O., Macchi, V., Porzionato, A., & De Caro, R. (2014). The infrapatellar fat pad and its role in knee biomechanics and pain. Journal of Anatomy, 224(2), 147–155.
Neurophysiology of HVLA and LVLA – Mechanisms and Stepwise Approach

Lumbar Spine Mobility Assessment and Facet Joint Analysis
In the Orthopedic Massage for Spine Mobility and Breathing course at RSM International Academy,
HVLA (High-Velocity Low-Amplitude) and LVLA (Low-Velocity Low-Amplitude) joint manipulation are taught for pain reduction, postural improvement, functional recovery and sports performance with an emphasis on safety and neuromuscular re-education.
To optimise joint motion, the therapist first assesses misalignment caused by muscle tension, trigger points and fascial restriction, while palpating during massage and observing the kinetic chain through guided stretching to identify movement dysfunction.
HVLA is never performed abruptly. Treatment begins with superficial myofascial release and active soft-tissue release, followed by deep-layer soft-tissue release around the joint to reduce tension. Then, LVLA joint mobilisation restores physiological motion and promotes joint centralisation.
This sequence stimulates capsular mechanoreceptors (Types I & II), enhancing neural glide, joint position sense, and coordination. LVLA specifically facilitates postural control and sensory reintegration. RSM follows the principle “Release → LVLA → Minimal HVLA.”
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
RSM International Academy
References
1) Bialosky JE et al. (2009). Manual Therapy, 14(5), 531–538. [PubMed ID 19539559]
2) Pickar JG. (2002). Spine Journal, 2(5), 357–371. [PubMed ID 14589477]
Reed WR et al. (2020). Clinical Biomechanics, 73, 86–92. [PubMed ID 31958668]
3) Sterling M, Jull G. (2001). Manual Therapy, 6(3), 139–148. [PubMed ID 11414774]
Clinical Application of HVLA and LVLA – Safety and Evidence
Lumbar Spine Facet Joint Biomechanics
At RSM International Academy, safety and patient specificity take priority in choosing between HVLA and LVLA.
For elderly or high-BMI clients with bone spurs, HVLA may detach micro-fragments and irritate nerves, so RSM uses a protocol centred on myofascial release, deep-tissue massage, and LVLA-dominant mobilisation.
HVLA is never performed on the cervical spine. Instead, alignment is corrected via deep-tissue methods, myofascial release, and towel-assisted LVLA traction for safe motion re-education.
In joint-manipulation sessions co-hosted with the Faculty of Medicine, Chiang Mai University, professors shared clinical examples:
“When HVLA is applied to osteophytic segments, small bone fragments may migrate and compress nerves—hard to detect on MRI and very difficult to remove surgically.”
Based on these clinical findings, RSM strictly follows the stepwise protocol “Release → LVLA → Minimal HVLA.”
This approach naturally induces pain relief, range-of-motion recovery, and neuromuscular re-education,
enhancing post-surgical rehabilitation and athletic performance with minimal post-session soreness and sustained results.
- Hironori Ikeda, MSc Sports Medicine
Manual Therapy & Neuro-Myofascial Release Specialist
References
1) Puentedura EJ, Louw A. (2012). Physical Therapy, 92(7): 1097–1110. [PubMed ID 22654195]
2) Gorrell LM, Beffa R, Christensen MG. (2019). J Manipulative Physiol Ther, 42(1): 25–33. [PubMed ID 30509569]
3) Bialosky JE et al. (2018). J Orthop Sports Phys Ther, 48(9): 656–664. [PubMed ID 30126184]
Synchronizing Body Axes and Center of Gravity through Balance Ball Training
The Relationship Between Pelvic Nutation, Counternutation, and Center of Gravity
The essence of Sports Medicine-Based Performance Training lies in mastering the synchronization between the body’s gravitational center (COG) and the central axis of unstable surfaces, such as balance or BOSU balls. This process defines true postural alignment: by aligning the kinetic chain with the ball’s fluctuating center, practitioners establish stability through motion, not stillness. It is a process of neuromuscular calibration, where each muscle group learns its precise contribution to whole-body equilibrium.
Within the Dynamic Postural Assessment framework of RSM International Academy, this synchronization process re-educates the kinetic chain through movement transitions—from static to dynamic and dynamic to static. By refining proprioceptive sensitivity and fascial tension distribution, practitioners cultivate a conscious awareness of their Body Axis Alignment. This enhances control in sport-specific actions, reduces compensatory patterns, and improves motor efficiency.
In clinical and athletic settings alike, this synchronization is essential not only for postural correction but also for pain management and rehabilitation. Once the kinetic chain becomes functionally integrated, the athlete achieves both mechanical efficiency and movement fluidity—hallmarks of high-level sports medicine practice.
- Hironori Ikeda, MSc Sports Medicine
Neurodynamics & Sports Biomechanics Specialist
References:
1) Willardson, J.M. (2007). Core stability training: applications to sports conditioning programs. Journal of Strength and Conditioning Research, 21(3), 979–985.
2) Panjabi, M.M. (1992). The stabilizing system of the spine. Part I: Function, dysfunction, adaptation, and enhancement. Journal of Spinal Disorders, 5(4), 383–389.
