
RSM Blog: Manual Therapy Techniques
Myofascial Release for Plantar Fasciitis

Dynamic Myofascial Release Course for sports injury
Many therapists overlook the plantar fascia's dynamic role within the Superficial Back Line. When teaching the Dynamic Myofascial Release Course at RSM International Academy, I frequently remind students that pain located in the heel is rarely a localized issue; it is a downstream consequence of upstream dysfunction. When patients present with the sharp, stabbing sensation characteristic of this condition, the temptation is to treat the foot in isolation. However, effective myofascial release for plantar fasciitis requires a comprehensive understanding of the kinetic chain, specifically the relationship between the calf complex, the calcaneus, and the plantar structures.
A focused, sports-medicine-based approach does not simply aim to reduce symptoms. It seeks to restore the sliding capacity of the fascial layers and correct the biomechanical load that caused the irritation.
Biomechanics of Plantar Fasciitis
To treat this effectively, we must understand the mechanics. The plantar fascia is a dense aponeurosis originating from the calcaneus and attaching to the phalanges. It acts as a tie-rod for the longitudinal arch via the Windlass Mechanism. During the push-off phase of gait, the toes extend, tightening the fascia and raising the arch to create a rigid lever for propulsion.
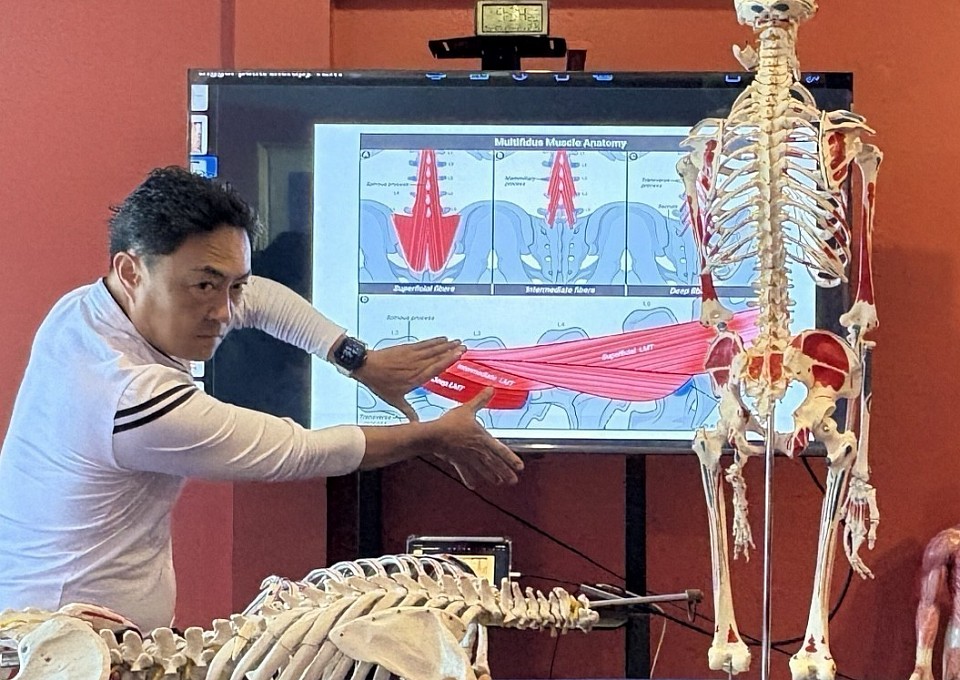
Dysfunction arises when this mechanism is disrupted. Often, the primary driver is the triceps surae – the gastrocnemius and soleus muscles. Because the Achilles tendon paratenon is continuous with the plantar fascia, extreme tension in the calf exerts a constant pulling force on the calcaneus. This traction force keeps the plantar tissue under strain, even at rest. Over time, this chronic load leads to micro-tearing at the insertion point.
The body responds with inflammation and collagen degeneration. While the term “fasciitis“ implies active inflammation, chronic cases are often “fasciosis,” a state of tissue degradation. This distinction is vital because anti-inflammatory medication addresses pain but fails to correct the tensile load degrading the tissue.
Why Manual Therapy Is Necessary
Standard stretching protocols often fail because they treat the tissue as a single elastic band. Fascia is a complex matrix that relies on hydration to slide. When tissue is immobile, the ground substance becomes viscous, creating densification. Simple stretching cannot resolve densification; it merely pulls at the ends of a knotted rope.
Myofascial release targets these densifications directly. By applying shearing forces, a therapist generates heat and friction to change the viscosity of the ground substance from a gel-like state to a fluid state. This restoration of glide is paramount. Once the fascial layers slide over the muscle bellies, the tension on the calcaneal insertion drops immediately.
Patients often resort to a generic internet search for relief, finding advice ranging from cortisone injections to invasive surgery. While plantar fasciotomy is an option for recalcitrant cases, it permanently alters arch stability. In contrast, manual therapy preserves structural integrity while restoring function.
Clinical Protocols to Treat Plantar Dysfunction
At RSM, our approach to treat plantar pain involves a sequence that addresses the entire posterior chain before touching the painful spot. I discourage digging elbows directly into an inflamed heel immediately, as this often aggravates nociceptors and causes guarding.
Releasing the Posterior Calf
The treatment begins with the gastrocnemius and soleus. We identify trigger points in the medial head of the gastrocnemius, a common referral source for heel pain. Using slow melting pressure, we separate the gastrocnemius from the underlying soleus. Following this, we address the Achilles tendon using lateral shearing rather than deep pressure. Mobilizing the tendon side-to-side encourages freedom of movement at the calcaneal interface, providing slack to the plantar surface.
Addressing the Plantar Surface
Once upstream tension is managed, we move to the foot. The goal is to separate the central band of the fascia from the lateral and medial bands.
- Calcaneal Decompression: We use manual traction to pull the calcaneus posteriorly, away from the forefoot.
- Longitudinal Stripping: Using a knuckle, we apply slow strokes from the heel toward the toe. This encourages the lengthening of collagen fibers.
- Cross-Fiber Friction: To break down fibrotic nodules, we apply friction perpendicular to the fiber direction. This stimulates fibroblast activity and remodeling.
Self-Care and Fasciitis Release
Recovery is a partnership. To maintain clinical gains, the client must perform specific care routines. I often assign homework focusing on self-myofascial release.
A standard foam roller is often too large to effectively target deep calf muscles or the arch. A lacrosse ball is superior. For the calf, the patient sits on the floor with the ball under the tightest part of the soleus. They mobilize the ankle through its full range of motion while applying pressure. This “pin and stretch” technique mimics clinical manual therapy.
For the foot, rolling a frozen water bottle under the arch provides analgesic cooling and mechanical release. However, I advise against aggressive rolling directly on the painful insertion. The goal is to release plantar tension in the mid-foot, not to irritate the attachment point.
Passive release is rarely enough. The foot must be strong enough to support body weight. We utilize “short foot” exercises where the patient pulls the ball of the foot toward the heel without curling the toes. This activates intrinsic muscles, reinforcing the arch. Consistent engagement in sports requires this active stability.
Long-Term Prevention and Mobility
The resolution of fasciitis myofascial restrictions involves a lifelong commitment to mobility. Flexibility of the ankle joint is the primary metric we track.
Limited ankle dorsiflexion is a silent killer of foot health. If the ankle cannot bend sufficiently during gait, the foot is forced to pronate excessively to unlock the midtarsal joint. This compensatory pronation wrings out the fascia. Therefore, athletes must incorporate dynamic calf stretching into warm-ups and static stretching into cool-downs.
When we treat the body as a machine of interconnected parts, we stop chasing symptoms. The pain in the heel is a signal of mechanical failure elsewhere. By tracing the kinetic chain upwards, we usually find the culprit in tight calves or immobile hips. Effective treatment requires patience, as collagen remodeling takes time. However, by restoring viscoelastic properties through myofascial release, we offer patients a permanent solution rather than a temporary fix.
Sports Massage for Chronic Pain Management: Beyond Symptom Relief

Sports Massage for shoulder injury prevention
During practical training at RSM International Academy I often find students attempting to address long-standing discomfort at the specific site of pain. However, the problem may instead begin with a root mechanical fault – a restriction in joint mobility or a deep fascial adhesion – that forces the body to compensate.
In RSM's Sport Massage Course, we teach that a therapist must move beyond simple memorization of anatomical points. We must visualize the three-dimensional relationship between the nervous system, the fascial network, and the musculoskeletal structure. Chronic conditions are not simply acute injuries that failed to heal; they are physiological adaptations that require a distinct, targeted treatment approach.
Understanding Chronic Pain Neurophysiology
When discussing chronic pain, we must distinguish it from acute injury. Acute discomfort warns the body of immediate damage, whereas chronic conditions often involve a sensitized nervous system. This phenomenon changes how the body perceives sensory input.
If a localized injury is left untreated, the brain commands surrounding muscle groups to tighten in a protective guarding mechanism. This constant state of tension restricts circulation, leading to localized hypoxia. Hypoxic tissue becomes fibrotic, creating adhesions that further restrict movement. This leads to a self-perpetuating cycle: tension causes ischemia, ischemia causes pain, and pain causes more tension.
Treatment must interrupt this cycle. We cannot simply force the muscle to relax. We must alter the neurological input, convincing the nervous system that protective guarding is no longer necessary.
Sports Massage vs. Standard Massage Therapy Protocols
In the general wellness industry, massage therapy is often synonymous with relaxation. While relaxation lowers cortisol, it is rarely sufficient for resolving specific, long-standing dysfunction. Sports massage operates on different principles.
In a sports medicine context, we utilize specific techniques designed to manipulate soft tissue structurally. For example, we employ deep friction to break down scar tissue formed around a healed muscle tear. This type of massage is necessary to restore fiber elasticity.
Sports therapy focuses on functional outcomes. When a client presents with limited range of motion, light effleurage will not suffice. We must apply precise, deep pressure to separate fascial layers. This mechanical input stimulates mechanoreceptors, overriding nociceptive signals. Consequently, the brain receives new sensory data, allowing it to “reset” the resting tone of the targeted muscle.
We often observe that standard massage fails because it is too generalized. A therapist might treat the entire back but miss the specific adhesion causing the problem. Effective treatment relies on assessment. If we do not identify the structural cause, the massage acts merely as a temporary distraction rather than a corrective intervention.
Medical Massage Strategies for Pain Relief
Medical massage distinguishes itself by its specific application to diagnosed conditions. When seeking pain relief, the specificity of the treatment is paramount. We are engaging with the physiology of recovery.
One primary mechanism we utilize is ischemic compression. By applying sustained pressure to a hyper-irritable spot within a muscle, we temporarily occlude blood flow. When pressure is released, fresh, oxygenated blood floods the tissue. This process flushes out metabolic waste products that irritate nerve endings.
Deep tissue work also addresses the thixotropic properties of fascia. Under stress, the ground substance of fascia becomes viscous. The mechanical heat generated during a massage transforms this substance back into a fluid state. This restoration of glide is crucial for relief. However, deep pressure must be applied intelligently. If the pressure is too aggressive, the body will perceive it as a threat. We teach students to “melt” into the tissue to access deeper layers required for therapeutic change.
Treating Chronic Low Back Pain via the Kinetic Chain
Chronic low back issues are among the most common complaints we see. Yet, the lumbar spine is rarely the sole culprit. In many athletes and general clients, a simple restriction in the hip or ankle significantly influences back pain.
The thoracolumbar fascia links the upper and lower body. If the glutes are inhibited, the lower back muscles overwork to stabilize the spine. As a result, treating the lower back exclusively often results in the pain returning.
Effective massage for this region requires a kinetic chain approach. We often start by assessing the psoas major. A tight psoas pulls the lumbar spine into excessive arching, compressing facet joints. By releasing tension in the psoas, we often provide immediate relief to the back without touching the spine. Similarly, tight hamstrings pull down on the pelvis, flattening the lumbar curve. Massaging the hamstrings improves mobility and restores neutral alignment. This causal logic is the hallmark of advanced sports massage.
Integrating Pain Treatments and Long-Term Pain Management
Pain management is rarely achieved through passive treatment alone. While massage provides a window of opportunity by reducing tension and restoring circulation, the client must utilize that window to move. Recovery is an active process.
We emphasize that pain treatments must be part of a broader strategy. Once we have released soft tissue restrictions, the client must re-educate the neuromuscular system. If we loosen a tight shoulder but the client continues to sit with poor posture, the body will revert to its previous pattern. The massage resets the hardware; movement re-programs the software.
Therapeutic modalities like corrective exercise and hydrotherapy complement our manual work. In the context of chronic pain, we must also manage expectations. A flare-up does not necessarily mean the treatment failed; it may be the body adjusting to a new structural alignment.
Clients who engage in regular massage maintenance, viewing it as hygiene for their musculoskeletal system, experience fewer episodes of acute dysfunction. The goal is to keep tissue pliable and joints mobile. Through this lens, we elevate massage from a luxury to a vital component of healthcare. Whether dealing with back pain or repetitive strain, targeted massage techniques remain one of the most effective tools for long-term health.
Advanced Massage Techniques for Sports Injuries

Sports massage for injury prevention
Many practitioners view the treatment of athletic conditions as a simple application of pressure to a sore area, overlooking the critical role of the broader kinetic chain. A frequent correction I make during practical training, particularly in RSM core modules like the Trigger Point Therapy Course, involves students attempting to address a sports injury by solely focusing on the local site of discomfort. In my experience, effective treatment requires a deep understanding of anatomy, biomechanics, and the physiological cascade of structural repair.
At RSM, we emphasize that massage is not just a relaxation tool; it is a potent medical intervention. To truly master rehabilitation, a practitioner must move beyond simple memorization. They must visualize the three-dimensional relationship between force transmission and neurological feedback. This article explores the specific clinical approaches we teach to optimize recovery, manage physical distress, and restore function in high-performance individuals.
The Role of Massage Therapy in Sports Medicine
The integration of massage therapy into a sports medicine curriculum provides a distinct advantage in client management. While modalities like ultrasound have their place, manual work offers direct palpation of soft structures. This tactile feedback allows the clinician to detect subtle changes in tonus and fascial density that machines miss.
When a competitor trains, micro-trauma occurs within the contractile fibers. This is a normal part of adaptation. However, without adequate recovery, this micro-trauma accumulates, leading to hypertonicity and altered joint biomechanics. Regular sports massage interrupts this cycle by flushing metabolic waste, reducing sympathetic nervous system dominance, and mechanically separating adhering fibers.
We define the primary goal of clinical massage as the restoration of homeostasis. A method applied during the acute phase differs vastly from one used during the remodeling phase. Applying deep massage too early can exacerbate inflammation, while applying it too late may fail to break down fibrosis. Therefore, timing is as important as the mechanics of the stroke.
Understanding the Mechanism of Injury
To treat a condition effectively, one must understand its origin. Athletic traumas typically fall into two categories: acute traumatic (e.g., ankle sprain) or chronic overuse (e.g., tendinopathy). In both scenarios, the body initiates a response characterized by inflammation, proliferation, and remodeling.
During the inflammatory phase, the priority is protection using lymphatic drainage. As the body moves into the proliferation phase, fibroblasts lay down collagen to repair the breach. This new collagen is often disorganized. Without guidance, this matures into scarring that lacks tensile strength. Through specific mechanical forces applied via massage, we can influence the alignment of these collagen strands, ensuring the repaired area can withstand the demands of high-performance sports.
Critical Massage Techniques for Rehabilitation
At RSM, we teach a variety of modalities, but specific massage techniques stand out for their efficacy. These are targeted massage interventions designed to alter structure and neurological tone.
Effleurage and Petrissage
While basic, these strokes are vital for diagnosis and fluid dynamics. I teach students to use effleurage to scan the body for temperature variances, while petrissage mechanically pumps fluids through the venous and lymphatic systems. For a client with heavy, fatigued limbs, this hydraulic effect is essential for flushing metabolic byproducts.
Deep Transverse Friction
This is critical for addressing tendon issues. Developed by Dr. James Cyriax, this method involves applying force perpendicular to the fiber direction to prevent cross-linking between collagen strands. For conditions like tennis elbow, friction stimulates local hyperemia and promotes the formation of functional fibrosis. It is uncomfortable, yet necessary for proper structural restoration.
Trigger Point and Myofascial Release
Trigger points are hyper-irritable spots that refer symptoms to distant areas. By applying ischemic compression, we induce a reactive flush of oxygenated blood to restore normal length. Similarly, myofascial release uses slow, sustained pressure to melt adhesions between connective tissue layers. This is particularly effective for runners with iliotibial band syndrome.
Facilitating Recovery and Reducing Inflammation
Muscle recovery is the limiting factor in training volume. Sports massage plays a pivotal role here by modulating the inflammatory response. We utilize lymphatic drainage techniques to accelerate the removal of inflammatory exudate. Unlike standard massage, which targets the musculature, lymphatic drainage targets the interstitial fluid using extremely light pressure to draw excess fluid away from the affected site.
Furthermore, massage therapy influences the autonomic nervous system. High-intensity training shifts a competitor into a sympathetic “fight or flight” state. Recovery occurs in the parasympathetic “rest and digest” state. Rhythmic, slow-paced massage stimulates the vagus pathway, lowering cortisol levels and enabling protein synthesis.
Strategies for High-Impact Sports & Joint Stability
Different sports impose unique demands. Runners load the posterior chain, often requiring deep stripping of the calf musculature to restore dorsiflexion and prevent Achilles tendinopathy. Conversely, overhead athletes (swimmers, tennis players) often suffer from anterior dominance. Here, massage focuses on releasing the pectoralis minor to open the subacromial space.
Regarding joint stability, static stabilizers (ligaments) are slow to heal due to poor blood supply. We teach “ligament stimulation”, using cross-fiber friction to stimulate fibroblast activity in injured bands. However, we must be careful with the Anterior Cruciate Ligament (ACL). While we cannot massage the ACL directly, we treat the surrounding musculature, specifically the hamstrings, which act as the primary dynamic stabilizer for the knee.
Advanced Sports Injury Massage Protocols
Developing a protocol for sports injury massage requires systematic assessment: History, Observation, Palpation, and Motion Testing.
- Acute Phase (0-72 hours): Manage edema and protect. Use Manual Lymphatic Drainage proximal to the site. No deep pressure.
- Sub-Acute Phase (3 days - 3 weeks): Organize fibrosis. Use gentle effleurage and light friction at the periphery.
- Chronic/Remodeling Phase (3 weeks+): Restore strength. Use deep transverse friction on scarring and active soft tissue mobilization.
- Maintenance: Identify compensation patterns. Perform a full kinetic chain assessment and deep work on compensatory areas.
Neural Gliding and Training Cycles
A frequently overlooked component is the nervous system. Neural pathways must glide between mechanical interfaces. If a pathway becomes entrapped by scarring, it generates “neural tension” that mimics muscle tightness. For example, recurrent hamstring tightness is often the sciatic nerve protecting itself. We use neural mobilization techniques to “floss” the nerve through its sheath.
We also adjust our therapy based on the athlete‘s schedule:
- Pre-Event: Fast-paced tapotement to stimulate the nervous system.
- Post-Event: Slow, compressive effleurage for recovery.
- Maintenance: Deep work and biomechanical corrections during training blocks.
The RSM Philosophy on Pain and Healing
At RSM International Academy, we teach that physical symptoms are messengers. Suppressing these signals without addressing the cause leads to dysfunction. When a client complains of discomfort, we ask: “What is this signal telling us about the load this body is under?”
We avoid the “no pain, no gain” mentality. While techniques like friction are uncomfortable, therapeutic pressure should always feel “constructive.” If the client tenses up, the massage is too deep, and the system is resisting. We also emphasize the psychological aspect of recovery. By explaining the mechanism of repair, we empower the client to become an active participant in their rehabilitation.
The Benefits of Regular Sports Massage
Beyond treating sports injuries, consistent massage therapy offers cumulative benefits.
First, it improves proprioception; the body’s ability to sense its position. When muscles are tight, signals become distorted. Massage sharpens this awareness. Second, it optimizes the length-tension relationship of the musculature, ensuring contractile units generate maximum force. Finally, the relaxation response lowers global stress, improving sleep. Sleep is the single most important factor in healing and performance.
Elevating the Standard
The field of sports medicine is evolving rapidly. Massage therapy must evolve with it. The modern practitioner must be a biomechanical detective and a recovery strategist.
Whether dealing with a weekend warrior or an elite athlete, the principles remain the same: respect the anatomy, facilitate natural healing, and treat the human, not just the part. By mastering these advanced concepts, therapists can deliver results that ensure long-term health and peak performance.
Key Takeaways for Practitioners
- Assess the Kinetic Chain: Look for root causes in joints above and below the site of symptoms.
- Respect the Phases: Match technique to the acute, sub-acute, or chronic stage.
- Mobilize Neural Pathways: Use neural gliding for restrictions that mimic muscle tightness.
- Educate the Client: An educated client adheres better to protocols.
- Consistent Maintenance: Prevent micro-trauma from becoming a macro-issue.
The Science of Sports Massage for Injury Prevention
Sports Massage for Injury Prevention
From Reactive Treatment to Proactive Care
Many therapists view bodywork strictly as a reactive measure, a tool deployed only after pain manifests or distinct pathology arises. In RSM's Sports Massage Course, we dismantle this perspective. We teach that the primary value of manual therapy lies not in fixing what is broken, but in maintaining the mechanical integrity of the musculoskeletal system to stop breaks from happening. Sports massage for injury prevention is a clinical discipline. It requires a deep understanding of anatomy, biomechanics, and the specific physiological demands placed on an athlete.
When I observe students during practical training, they often focus solely on the “complaint”, the tight hamstring or the sore shoulder. However, a sports medicine approach requires us to look at the variables preceding the symptom. We must ask what mechanical inefficiencies are loading that hamstring. By addressing these root causes through targeted manipulation, we interrupt the cycle of dysfunction before minor deviations escalate into debilitating conditions.
Physiological Mechanisms of Sports Massage
To effectively utilize bodywork for prevention, one must understand how it influences the body at a cellular and systemic level. Manipulating soft tissue initiates a cascade of mechanical and neural responses that directly counteract the stressors of high-level activity.
Managing Muscle Tension Before It Becomes Pathology
Hypertonicity, or excessive resting tone, is a silent precursor to many injuries. When a muscle group remains in a chronically shortened state, it exerts constant traction on its tendinous attachments. This constant pull creates micro-trauma at the insertion point, leading to tendinopathy.
In my clinical experience, I frequently see this in the quadriceps of cyclists. The rectus femoris remains tight, pulling upward on the patella even during rest. This alters patellar tracking. If we intervene early with specific massage protocols to normalize tone, we reduce that traction. We restore the optimal length-tension relationship of the contractile tissue. As a result, joint mechanics normalize, and the risk of patellofemoral pain syndrome diminishes.
Addressing Muscle Soreness and Facilitating Recovery
Delayed Onset Muscle Soreness (DOMS) and general fatigue are inevitable byproducts of intense physical exertion. While inflammation is a necessary part of adaptation, excessive inflammation can impede recovery. This leads to compensatory movement patterns. An athlete running with sore calves will subconsciously alter their gait, shifting loads to the hips or lumbar spine, creating a new potential injury site.
Through massage techniques that enhance venous return and lymphatic drainage, we manually flush metabolic byproducts from the interstitial spaces. This mechanical pumping action accelerates the delivery of oxygenated blood to repairing fibers, shortening the window of vulnerability where compensation occurs.
Effective Massage Techniques for Prevention
Not all manual therapy is created equal. General relaxation strokes have their place, but they rarely correct the structural adhesions that predispose an athlete to harm. At RSM, we emphasize technical precision.
Deep Tissue Interventions for Fascial Adhesions
The sliding surfaces between muscle layers are critical for fluid motion. Fascia relies on hydration to remain pliable. When tissues are immobile or overloaded, the hyaluronic acid between fascial layers becomes viscous, leading to densification and adhesions.
Using deep tissue strategies, we generate shear forces that restore the glide between these layers. For example, the interface between the gastrocnemius and the soleus is a common site of adhesion in runners. If these two muscles cannot slide past one another, the Achilles tendon absorbs erratic torsional loads. By manually separating these compartments, we ensure force transmission remains linear and efficient.
Myofascial Release and Trigger Points
Localized areas of sarcomere contracture, or trigger points, compromise a muscle’s ability to lengthen. A muscle that cannot lengthen fully is prone to tearing under eccentric load. We train our therapists to identify taut bands and apply ischemic compression to reset the local nervous tone. Once the trigger point is deactivated, we immediately take the joint through its full range of motion to re-educate the neuromuscular system.
The Role of Sports Medicine in Assessment
Integrating sports medicine principles shifts the focus from “rubbing muscles” to “optimizing performance.” A core component of this approach is the Dynamic Postural Assessment. We cannot prevent a sports injury if we do not know where the risks lie.
If we identify that a client has limited ankle dorsiflexion, we know the kinetic chain will force the foot to pronate excessively. This drives the tibia into internal rotation and stresses the medial knee. A standard massage might ignore the ankle. A preventative approach focuses intensely on the soleus and plantar fascia to restore dorsiflexion. By fixing the root, we protect the knee.
Correcting Muscle Imbalances
High-performance athletes operate at the limits of their capacity, where minor muscle imbalances are magnified. The relationship between agonist and antagonist muscles is often skewed by repetitive training.
Consider a swimmer’s shoulder. The pectorals and lats become strong and short, while the external rotators become weak. This pulls the humeral head forward, impinging the supraspinatus. Therapy here is not about relaxing everything. We must lengthen the pectorals while stimulating the external rotators. We use techniques that inhibit tone in overactive tissues and facilitate activation in weak ones. This restoration of balance centers the joint, ensuring it wears down slower.
Integrating Physical Therapy Concepts
The line between massage therapy and physiotherapy is becoming increasingly blurred. We use massage to prepare the tissue for the loading protocols prescribed by physiotherapists.
If a physical therapy protocol requires eccentric loading, the tissue must be compliant enough to handle that stress. If the hamstring is fibrotic, exercise may cause further tearing. We use manual therapy to align collagen fibers, ensuring that rehabilitation or pre-habilitation exercises are effective. We are the architects preparing the foundation upon which strength is built.
Designing a Periodized Therapy Plan
Prevention is a process, not a one-time event. Just as an athlete follows a periodized training schedule, they require a periodized treatment schedule.
- Pre-Season (Structural Correction): We use aggressive techniques to correct deep-seated dysfunctions, such as pelvic tilts or scar tissue, ensuring a balanced chassis.
- In-Season (Maintenance): Intensity drops. We focus on flushing edema and managing tone to address acute issues before they become pain patterns.
- Post-Season (Regeneration): We focus on total relaxation and neural down-regulation to allow the sympathetic nervous system to reset.
The Reality of the Kinetic Chain
I often explain to clients that the site of their pain is rarely the source of their problem. The body is a continuous system of linkages. If one link is rigid, the force is absorbed by the next link, causing wear and tear.
Sports massage acts as the mechanic for these links. By ensuring every joint moves freely, force is distributed rather than concentrated. A restriction in the thoracic spine forces the lumbar spine to compensate, leading to low back pain. Treating the back provides temporary relief; mobilizing the thoracic spine solves the problem.
At RSM International Academy, we believe sports massage is a requisite for longevity in sports. By managing muscle tension, correcting imbalances, and respecting the kinetic chain, we allow the body to function as designed. This clinical precision is what keeps athletes in the game.
Shiatsu and Meridian Energy Channels: Bridging Tradition and Anatomy

Deep Shiatsu Massage and Sports Medicine
In Western sports medicine, we are trained to isolate. We dissect the body into insertions, origins, and lever arms to understand the mechanics of injury. However, after years of clinical practice and teaching I have found that isolation often fails to explain chronic pain. This is where the understanding gained in RSM's Shiatsu Massage Course can provide a missing link.
Many therapists dismiss “energy lines” as esoteric. I challenge this view. When we overlay the map of shiatsu meridians onto modern anatomical charts, specifically the myofascial lines, the correlation is undeniable. The pathways mapped thousands of years ago often trace the exact routes of deep fascial planes and neurovascular bundles. For the elite therapist, shiatsu offers a diagnostic framework that sees the body as a continuous circuit rather than a collection of parts.
Defining Shiatsu and the Role of Meridians
To master this modality, we must strip away the mysticism and look at functional definitions. Shiatsu is a Japanese manual therapy evolved from traditional Chinese medicine (TCM). Unlike general massage, which focuses on kneading muscle bellies, this technique applies perpendicular pressure to specific points along defined pathways.
These pathways are the meridians. While traditional texts describe them as channels for Ki (or Qi), a clinical interpretation aligns this energy with the body’s bio-electric vitality and the autonomic nervous system. The body possesses a complex network of these channels connecting the interior organs (viscera) to the exterior structure (skin, muscle, bone).
I often explain to students that a meridian acts like a fiber-optic cable carrying information. If that cable is compressed, the signal degrades, manifesting as pain or dysfunction. Acupuncture points, located along these channels, typically lie at fascial cleavage planes – areas where connective tissue sheets diverge – allowing us to access the deep interstitial environment.
The Mechanics of Energy Flow
The health of a client depends on the uninterrupted movement of resources, described in TCM as smooth energy flow. Physical trauma or stress disrupts this current, creating areas of excess (Jitsu) or deficiency (Kyo).
In my experience, Western therapy often targets the Jitsu; the tight, painful knot. We attack the tension. However, the Jitsu is often just a symptom; a dam created by a lack of flow elsewhere. The Kyo, or empty area, is frequently the root cause. By restoring resources to the under-active area, the tension releases spontaneously. This systemic balancing act is the core objective of our treatment.
Navigating the Meridian Lines
The system comprises twelve primary meridian lines that run vertically across the body, categorized into Yin (solid organs, storage) and Yang (hollow organs, processing) pairs. This pairing is critical for maintaining balance. A dysfunction in a Yin organ often manifests as symptoms in its paired Yang partner.
The Kidney Meridian and Structural Stability
One of the most vital channels for athletes is the kidney meridian. Anatomically, this line begins at the sole of the foot, travels up the inner ankle, and ascends through the lumbar spine. Its trajectory mimics the Deep Front Line in myofascial anatomy, which is responsible for core stability.
When I treat athletes with chronic lower back pain, I almost invariably find weakness along this pathway. By stimulating specific points along the kidney meridian, specifically around the medial malleolus, we can often facilitate a release in the lumbar region without touching the back. This demonstrates the power of distal healing: solving a proximal problem by addressing a distal connection.
Identifying and Treating Energy Blockages
The goal of a session is to identify and remove energy blockages. A blockage acts like a logjam; above it, pressure and inflammation build, while below it, tissue becomes weak and cold.
Detecting these requires refined palpation. We look for energy “Tsubo” (points). In acupuncture, needles are inserted here; in shiatsu, we use body weight. Effective therapy requires the practitioner to lean into these points using gravity rather than muscular force. This generates deep, stationary pressure that invites the parasympathetic nervous system to respond, facilitating healing rather than guarding.
Conclusion: Integrating East and West
At RSM, we do not view Western sports medicine and Eastern traditions as opposing forces. Western medicine excels at acute repair; meridians excel at understanding functional relationships.
Integrating this knowledge transforms a standard routine. It allows the therapist to assess globally and restore homeostasis. By studying shiatsu, we gain a three-dimensional perspective, seeing the links between the ankle and the kidney, or the emotions and the organs. We stop treating symptoms and start treating the system, ensuring our treatment promotes long-term wellbeing.
Myofascial Release for Chronic Pain: A Clinical Approach

Dynamic Myofascial Release Course Chiang mai
Many therapists view pain as a local event, assuming that the site of the symptom is the source of the problem. In my experience teaching at RSM International Academy, this is the most common error in manual treatment. The body functions as a tensegrity structure where tension distributes across a continuous network. When this network fails to glide, the resulting dysfunction often creates chronic pain that defies standard treatment.
The failure usually resides within the myofascial tissues. While standard protocols often prescribe compression for these areas, compressing a glued layer of tissue rarely unglues it. To resolve these complex cases, students in our Myofascial Release Course learn to move beyond simple muscle manipulation and address the mechanics of the fascial matrix.
Understanding Myofascial Tissues in Dysfunction
To treat effectively, we must define what we are touching. The fascial system is a continuous web of connective tissue surrounding every muscle, nerve, and organ. It provides structural integrity and permits the sliding required for functional movement.
Under normal conditions, this system is fluid. However, trauma, inflammation, or repetitive stress alters the viscosity of the extracellular matrix. The fluid becomes gel-like, a phenomenon called densification. This restricts the sliding potential between layers.
When myofascial layers lose their glide, the kinetic chain suffers. A restriction in the thoracolumbar fascia transmits tension upward to the neck or downward to the glutes. Consequently, a client may feel neck stiffness that is actually a compensatory price for lower back immobility. Addressing the neck alone offers only temporary relief because the mechanical anchor remains. This explains why many clients cycle through physical therapy without lasting resolution.
The Science of Myofascial Release Therapy
Myofascial release therapy operates on different physiological principles than Swedish or Deep Tissue massage. The goal is not relaxation but the mechanical restoration of elasticity.
Two primary mechanisms drive this therapy:
- Piezoelectricity: Mechanical pressure generates a small electrical charge in collagen, signaling fibroblasts to remodel tissue along stress lines.
- Thixotropy: Sustained pressure changes the ground substance from a dense gel to a liquid state, restoring glide.
To achieve this, the therapist must engage the barrier and wait. Myofascial release is not about forcing through tissue; it is about melting restriction. If a therapist pushes too hard, the body’s protective reflex activates, causing the muscle to guard. Conversely, applying the correct drag allows the nervous system to downregulate, facilitating a deeper release.
Differentiating Trigger Points from Fascial Restrictions
While often found together, myofascial trigger points and fascial restrictions are distinct. A trigger point is a hyperirritable spot within a taut muscle band. A fascial restriction is a thickening of the connective web itself.
You cannot “press” a fascial restriction away like a myofascial trigger. Instead, the fascia requires elongation and shear. Often, trigger points are secondary to fascial tightness. If the fascial envelope is rigid, it increases internal pressure on the muscle, reducing blood flow. This hypoxic environment breeds trigger points. Therefore, addressing the fascial tension first often causes the trigger points to spontaneously resolve, making this a superior strategy for relieving pain.
Clinical Application and Pain Management
In sports medicine, we view myofascial work as a necessity for injury prevention. Athletes subject their bodies to repetitive loads that create specific patterns of densification. A sprinter may develop restrictions in the posterior chain that simple stretching cannot address because stretching pulls the whole chain rather than isolating the adhesion.
Effective pain management involves identifying these specific adhesion points. By freeing the interface between muscle groups, for example the septum between the quadriceps and hamstrings, we restore independent movement. This reduces chronic pain by removing the mechanical drag on the kinetic chain.
However, this approach is not limited to athletes. The desk worker with back pain often suffers from the same mechanism: the thoracolumbar fascia becomes matted down due to prolonged sitting. MFR re-introduces movement into that dense sheet of tissue.
MFR: A Precision Instrument
Transitioning from a massage therapist to a clinical practitioner requires seeing the body as a unified hydraulic system. Myofascial release is the tool that allows us to intervene in that system effectively.
By understanding the anatomy of the fascial network, we achieve outcomes that standard massage cannot. Whether treating a high-level athlete or a patient with pain syndrome, the objective remains the same: restore the glide and let the body heal. This leads to lasting relief and true structural correction. Through these precise techniques, we do not just treat tissues; we restore the architecture of movement.
Mastering Body Mechanics for Massage Practitioners
Functional Anatomy for Posture Correction
One of the most frequent corrections I make during practical training at RSM International Academy involves the therapist’s movement strategy rather than the specific technique. I often observe students attempting to generate pressure by isolating muscles in their arms and shoulders. They push with their triceps and strain their upper trapezius, an inefficient approach that creates a direct path to burnout. In our Deep Tissue Massage Course, we emphasize that a therapist’s greatest tool is the integrated use of their entire body. Sustainable, precise massage therapy is born from superior body mechanics.
This is not a matter of simple comfort; it is a requirement for a long career. The repetitive nature of massage work places significant biomechanical demands on the practitioner body. Without a deep understanding of leverage and weight transfer, therapists pay a physical price. Pain often starts in the thumbs or wrists before migrating to the shoulders and manifesting as chronic back pain. This physical degradation compromises the quality of the massage, leading to inconsistent pressure and reduced effectiveness.
Why Body Mechanics are Non-Negotiable for Massage Therapists
The career of a massage practitioner is physically demanding, similar to that of an elite athlete. However, while an athlete’s career is often short, a massage therapist aims for decades of practice. This longevity is impossible without mastering body mechanics. Poor mechanics force the smaller, vulnerable muscles of the upper body to do the work that should be performed by the large, powerful muscles of the legs and core.
This reliance on upper body strength leads to rapid fatigue. As fatigue sets in, form deteriorates, increasing the load on wrists and shoulders. From a sports medicine perspective, this is a dysfunctional movement pattern. The brain learns an inefficient way to perform a task, and this pattern becomes ingrained. Consequently, the therapist’s ability to deliver effective massage therapy diminishes. Proper body mechanics act as a preventative strategy, protecting the therapist’s health while ensuring professional viability.
The Core Principles of Force Generation and Control
Effective massage relies on generating force without muscular strain. This requires a shift from “pushing” to “leaning.” The primary source of power must be body weight and gravity. When a practitioner uses their body as a single unit, they can produce deep, consistent pressure without fatigue. The hands and forearms become simple conduits for force generated from the ground up.
This approach requires conscious control over the center of gravity. By shifting weight from the back foot to the front foot, a therapist creates a smooth, powerful stroke. The movement originates from the legs, travels through a stable core, and extends into the arms. The upper body remains relaxed, acting as a channel rather than a generator of force. This principle protects the small joints of the hands and wrists from cumulative stress.
The Critical Importance of Table Height
Before a session begins, the most important factor to establish is correct table height. An improperly adjusted massage table forces the therapist into a compromised posture immediately, disrupting the kinetic chain.
The ideal table height depends on the practitioner’s body and the specific therapy. A common guideline is setting the table to knuckle height when arms hang at the sides. However, this varies based on the technique:
- For deep tissue or sports massage, a lower table height allows the practitioner to use their body weight effectively, leaning into strokes with straight arms.
- For lighter techniques, a slightly higher table reduces the need to bend over.
If the table is too high, the practitioner must abduct their shoulders to apply pressure, engaging the upper trapezius and causing neck pain. Conversely, if the table is too low, the practitioner must bend at the waist, placing strain on the lumbar spine. Finding the precise table height preserves the health of your back and shoulders.
Generating Pressure Without Compromising Your Back
The lower back is vulnerable for massage therapists. Leaning over a table creates constant flexion load on the lumbar spine. If a therapist generates pressure by pushing from their back, this load increases, raising the risk of injury. The key is to maintain a neutral spine and generate force from the legs.
This begins with the stance. A therapist should use a lunge stance, also known as the archer stance, with one foot forward and one back. This creates a wide base of support. The movement for a stroke becomes a rock forward and back, not a bend at the waist. The spine remains aligned, a concept known as “stacking the joints.” This ensures force transmits through the skeleton rather than being absorbed by back muscles.
When deep pressure is needed, the therapist should sink their weight by bending at the knees and hips, keeping the back straight. This engages the glutes and quadriceps. The core muscles must engage to stabilize the pelvis. By treating the core as the center of movement, a therapist delivers powerful pressure without sacrificing their back health.
Achieving Proper Body Alignment
From a biomechanical standpoint, correct body alignment means stacking joints to transfer force efficiently. For a massage practitioner, this alignment separates a healthy career from one cut short by strain. We teach students to build posture from the ground up.
The Feet and Stance
Everything starts with the feet. They are the foundation. An unstable base creates compensations throughout the body. With feet shoulder-width apart and one foot forward, the lunge stance provides stability. The back foot acts as the anchor, while the front foot provides balance. Rocking from back to front allows the therapist to use body weight for momentum. This dynamic movement is essential for endurance.
Hips and Pelvis
The pelvis links the lower and upper body. To utilize the hips, a therapist must hinge at the hips rather than flexing the spine. When leaning into a stroke, the movement feels like a forward tilt of the pelvis, maintaining the lower back’s natural curve. This engages the glutes and hamstrings. A stable pelvis ensures force from the legs transfers efficiently to the hands.
Spine and Shoulders
The spine should remain in a long, neutral position. This avoids excessive rounding or arching. A neutral spine allows vertebrae to load evenly. Similarly, shoulders are prone to injury. A common mistake is allowing shoulders to elevate and round forward. This compromises the rotator cuff. Instead, shoulders should be kept down and back. This “packed” position creates a stable base for the arm, reducing impingement risk.
Applying Mechanics to Massage Techniques
Theoretical understanding must translate to practical execution. Each technique can be performed in a way that is either draining or sustainable. The goal is to integrate stance, weight transfer, and alignment into every movement.
Effleurage: The Art of Leaning
Effleurage is often where poor habits appear. Many therapists push with their arms. The correct method uses the lunge stance, leaning into the stroke by shifting weight to the front leg. Arms remain straight, acting as levers. Pressure is modulated by how much body weight is leaned into the stroke. The return stroke allows recovery as weight rocks back. This rhythmic movement uses gravity to generate consistent pressure.
Petrissage and Frictions
Techniques like petrissage require localized pressure. Generating this force with small hand muscles is a mistake. Power must come from the larger structures. The therapist should maintain a stable base. Force is generated by leaning body weight, directed through a contact point like the thumb or elbow. Hand joints should remain in neutral alignment. For example, the thumb should be supported by fingers to create a buttress. The movement comes from the body shifting, not isolated hand contraction. This application of proper body mechanics ensures specific work is delivered safely, preserving the practitioner body for years of practice.
Myofascial Release for Jaw Tension

Professional Sports Massage School
Students in our Myofascial Release Course often attempt to address upper cervical stiffness by focusing on the neck. They treat the symptoms visible on the posterior chain but ignore the primary driver located anteriorly. In my experience, the stomatognathic system, comprising the teeth, mandible, and associated soft tissues, acts as a silent dictator of upper body mechanics. When a therapist overlooks the masticatory muscles, they fail to resolve the root cause of the dysfunction.
Mechanical stress in the masticatory muscles frequently initiates a cascade of global postural issues. If the masseter and temporalis are locked in a concentric contraction due to bruxism, the reciprocal tension transmits directly into the suboccipital triangle. This mechanical coupling forces the head into a forward posture to maintain an open airway. Consequently, the trapezius and levator scapulae become hypertonic to support the leverage of the head. Treating the shoulders while ignoring jaw tension is effectively bailing water from a boat without plugging the leak.
Understanding TMJ Disorders and the Kinetic Chain
To treat dysfunction effectively, we must first understand the unique architecture of the temporomandibular joint. It is the only bilateral structure in the body that must move synchronously; a restriction on the left side instantly alters the biomechanics of the right. This dependency creates a scenario where a unilateral muscle spasm forces the contralateral side to overwork, eventually leading to a tmj disorder.
The masticatory system operates through a powerful sling mechanism. The masseter and medial pterygoid form a functional loop around the angle of the mandible. When these muscles are balanced, the mandible tracks centrally. However, if one component becomes short and fibrotic, it creates a shearing force across the disc.
In our curriculum, we also emphasize the Deep Front Line. This myofascial meridian runs from the deep structures of the foot, through the pelvic floor and diaphragm, terminating at the muscles of mastication. This pathway explains why I often observe a correlation between pelvic instability and clenching. A dysfunction at the top of this line theoretically influences pelvic stability and breathing mechanics. In a sports medicine context, this restriction can limit diaphragmatic excursion, reducing VO2 max potential in endurance athletes simply because the upper chain is locked.
The Anatomy of Orofacial Pain
The term orofacial pain encompasses a wide spectrum of symptoms, but in a manual therapy context, we look specifically for myofascial trigger points and entrapments. The culprit is rarely a single muscle. Instead, it is a synergistic failure of the muscles of mastication.
The masseter is the strongest muscle in the human body relative to its size. When it becomes hypertonic, it develops distinct trigger points that refer sensation to the ear and the upper molars. Clients often mistake this for a toothache. Conversely, the temporalis acts as the “positioner” of the mandible. Trigger points in the temporalis refer sensation into the temple and above the eye, often mimicking tension headaches.
Fascia is not merely a wrapping; it is a sensory organ. In the face, the fascia is exceptionally dense. Persistent clenching causes this tissue to densify and dehydrate. The hyaluronic acid between fascial layers becomes viscous, turning from a lubricant into a glue-like substance. This inhibits the smooth gliding required for the condyle to translate forward. Chronic dysfunction here leads to structural changes within the capsule itself. Therefore, simply stretching the area is ineffective. We must apply shear force to the fascia to restore hydration and glide.
Moving Beyond Standard Myofascial Massage
Standard education often glosses over the face, treating it as a “cosmetic” zone rather than a functional one. However, effective myofascial massage for the masticatory system requires a high degree of precision. We cannot simply knead the cheek. We must visualize the fiber direction and the depth of the layers.
Treating the exterior muscles is only half the equation. The lateral pterygoid is perhaps the most clinically significant yet least understood muscle in this region. It is the primary depressor and protractor of the mandible. Crucially, the lateral pterygoid inserts directly into the articular disc. Spasm in this muscle pulls the disc anteriorly, causing it to displace and creating the characteristic “click” or “pop.” Because the lateral pterygoid is tucked behind the zygomatic arch, it is difficult to palpate externally. This necessitates an intraoral myofascial approach.
Protocols for TMJ Release
TMJ release is not about forcing the mouth open. It is about down-regulating the nervous system and restoring space within the capsule. My clinical philosophy prioritizes the “less is more” approach initially. The trigeminal nerve is easily aggravated, and aggressive pressure can cause a protective muscle splinting response.
We apply myofascial release by engaging the restriction barrier with sustained, low-load pressure. We wait for the tissue to “melt” or yield. Using a gloved hand, the therapist enters the buccal cavity to locate the pterygoid pocket between the upper molars and the cheek. The goal is to apply a gentle lateral or superior distraction. This technique often produces an immediate reduction in facial tension and an increase in the range of motion. It resets the proprioceptors, allowing the nervous system to adopt a new, more relaxed “neutral” position.
Self-Myofascial Release for Maintenance
Since we cannot be with the client 24 hours a day, client education is paramount. I teach students to prescribe self-myofascial release techniques that are safe and effective. Without daily maintenance, the neuromuscular patterns that drive clenching will likely return.
One effective method involves the client using their own knuckles or fingertips to strip the masseter.
- Masseter Release: Place the heel of the hand or soft knuckles just under the cheekbone (zygomatic arch). Apply moderate pressure inward and slowly slide down toward the angle of the mandible while slowly opening the mouth. This active release technique pins the tissue while lengthening the muscle unit.
- Temporalis Release: Using flat fingertips, apply pressure to the temples. Instead of rubbing the skin, move the scalp over the skull. Look for tender spots and hold the pressure while opening and closing the mouth.
This self-care routine empowers the client. It breaks the pain cycle and provides them with a tool to manage stress-induced tightening before it becomes a full-blown spasm.
Developing the “Thinking Hands”
At RSM International Academy, the goal is not to produce robots who follow a script. The goal is to develop “thinking hands.” When you approach a case of jaw pain, you are not just rubbing a sore spot. You are interacting with a complex fulcrum that balances the cranium against gravity.
Mastering the stomatognathic system separates the average therapist from the clinical specialist. It requires a deep dive into osteology, myology, and neurology. But the reward is the ability to solve complex pain puzzles that have baffled other practitioners. By addressing the myofascial structures of the head and neck with precision and causal logic, we restore not just movement, but quality of life. The mandible is small, but its influence is massive. Treat it with the respect it commands.
How to Track Progress in Massage School

Sports Medicine Massage School
At RSM, we consistently emphasize to students at our massage school here in Thailand that achieving elite practitioner status is not determined by the quantity of hours spent practicing, but by the advancement of clinical reasoning skills. When students inquire about how to assess their development, I explain that genuine progress is reflected in their ability to integrate isolated anatomical knowledge into a comprehensive treatment strategy. Advancement is intellectual as well as physical.
The Evolution of Clinical Competence in Massage Therapy
During the early stages of training, students naturally concentrate on their own hands, focusing on the mechanics of pressure, rhythm, and sequence. However, this inward focus can impede clinical perception. A clear indicator of progress is when students shift their attention from their own actions to the client’s tissue response.
We specifically monitor this progression through the refinement of palpation skills. In the first month, a student may identify a general muscle group such as the hamstrings. By the third month, they should distinguish between the semitendinosus and biceps femoris muscles and detect specific adhesions within the intermuscular septum. This enhanced tactile acuity enables more precise interventions. Consequently, students transition from guessing to accurate assessment. The ability to trace dysfunction along the kinetic chain differentiates sports medicine-based massage therapy from conventional relaxation techniques.
Mastering the SOAP Note for Objective Tracking
Documentation remains the most concrete method for monitoring this developmental trajectory. The SOAP note serves not merely as administrative paperwork but as a diagnostic instrument that reveals the therapist’s clinical reasoning. Within our curriculum, we assess the quality of these notes to determine whether students have truly assimilated the material.
Subjective and Objective Data
The “Subjective” section reflects the student’s capacity to extract pertinent client history. A novice might record “shoulder pain,” whereas an advanced student documents “sharp pain in the supraspinatus tendon during abduction, relieved by external rotation.” This level of detail demonstrates an understanding of the injury mechanism. Similarly, the “Objective” section evaluates assessment skills, seeking precise measurements such as “Right cervical rotation limited to 45 degrees.” Without quantifying dysfunction in the notes, students cannot effectively measure treatment outcomes.
Utilizing Customizable SOAP Formats
Standard forms rarely capture the nuances essential in sports medicine. Therefore, we employ customizable SOAP templates that prompt students to perform specific orthopedic tests. By including fields for assessments like the Thomas test or Phalen’s test, students are compelled to evaluate before treating. This repetition fosters the habit of clinical testing, ensuring that every massage session is intentional and evidence-based.
The Role of Digital Notes Software
Contemporary practice demands modern tools. We introduce students to various digital notes software to enhance clinical tracking efficiency. The principal advantage of digital systems is the ability to visualize client progress over time. When students log sessions digitally, they can monitor changes in pain levels and range of motion (ROM) across weeks or months.
For example, platforms akin to MassageBook SOAP notes enable students to tag specific muscles on 3D body maps. This visual feedback loop is critical for learning. If data indicates no improvement in a client’s ROM after three sessions, students must reassess their treatment strategy. Recognizing the ineffectiveness of a plan is a pivotal learning moment. Additionally, familiarity with client management systems prepares students for the operational realities of clinical practice, facilitating seamless integration of scheduling and documentation.
Detailed Assessment as a Progress Indicator
The cornerstone of the RSM method is that treatment cannot be effective without thorough assessment. Therefore, a student’s progress is directly correlated with their assessment proficiency.
During client intake, I often observe students’ approaches. Beginners tend to rush to begin treatment, whereas advanced students dedicate time to observing gait, posture, and functional movement. They recognize that the underlying cause of pain frequently manifests in a client’s stance or movement patterns.
We evaluate progress by assessing the student’s “clinical eye.” Can they identify a pelvic tilt or restricted thoracic rotation? These observations must be meticulously documented in SOAP notes. When a student discerns that knee pain originates from hip restrictions, it alters the treatment approach. This causal reasoning enables students to move beyond symptom management toward addressing root causes.
Developing Effective Treatment Plans and Case Studies
A critical milestone in massage education is the ability to develop comprehensive long-term treatment plans. Novices typically address only immediate symptoms; professionals treat the entire organism over time.
We require students to design multi-session plans, demonstrating an understanding of the physiological timelines necessary for tissue repair. To reinforce these concepts, we utilize case studies. Students follow a single “client” through multiple treatments, compiling SOAP notes into a coherent clinical narrative.
- Initial Evaluation: Establishing baseline pain and functional status.
- Intervention: Documenting specific techniques applied.
- Outcome: Reassessing metrics to evaluate treatment efficacy.
- Research: Comparing findings with current literature.
By engaging with peer-reviewed research, students learn to anchor their practice in evidence-based methodologies. If a technique proves ineffective, they investigate alternatives. This commitment to self-directed learning serves as a vital safeguard for their professional careers.
Evaluating Technique Precision and Client Outcomes
While cognitive skills are paramount, the physical execution of massage remains the therapeutic vehicle. We assess technical proficiency through practical examinations, focusing on qualitative metrics such as body mechanics and the “listening hand.”
A student who becomes fatigued after two sessions has not yet mastered leverage. Progress is demonstrated by the ability to apply deep pressure efficiently, preserving therapist endurance. Additionally, we evaluate the student’s sensitivity to tissue resistance barriers. The skill to engage these barriers and await release distinguishes students prepared for graduation from those requiring further practice.
Ultimately, the most reliable indicator of progress is client outcome. We encourage students to view pain reduction not as the sole objective but as a byproduct of restored function. When clients report decreased pain alongside improved mobility, it signifies a functional success.
The Path to Mastery in Massage
Tracking progress in massage education necessitates a multifaceted approach. Passing exams alone is insufficient. Students must demonstrate the ability to synthesize assessment data, formulate logical treatment plans, and execute precise techniques. Through rigorous SOAP documentation and a steadfast commitment to clinical reasoning, students evolve into practitioners capable of resolving complex dysfunctions.
At RSM International Academy, we do not merely teach massage; we cultivate the discipline of sports medicine. By meticulously tracking anatomy, biomechanics, and client responses, our students ensure continuous improvement. This commitment to daily progress is the true measure of success.
Adapting Massage for Elderly Clients with Sports Medicine Principles

Sports Medicine Massage Course
I sometimes observe students in our Deep Tissue Massage Course attempting to address age-related musculoskeletal dysfunction by focusing on reducing pressure. They assume that fragility equals a need for inactivity or purely superficial touch. While caution is necessary, this binary view overlooks the complex physiological reality of the aging body. In my experience as a Sports Medicine specialist, I have found that effective massage therapy for this demographic requires a sophisticated understanding of sarcopenia, hemodynamic stability, and connective tissue fibrosis. We do not simply “go light”; we adjust our mechanics to match the altered biological landscape of the patient.
Understanding Physiological Changes in the Older Body
To provide effective care, a practitioner must first understand the substrate they are working on. The process of getting older is not merely a chronological marker; it is a cascade of physiological changes. The most significant of these is sarcopenia, the involuntary loss of skeletal muscle mass. As muscle fibers atrophy, the protective padding over bony prominences diminishes, leaving nerves and vasculature exposed.
Consequently, standard deep tissue pressure using elbows or thumbs becomes clinically contraindicated in many areas. The force a healthy quadricep can absorb will damage the atrophied tissue of an 80-year-old. This leads to a necessary shift in tool selection. We transition to broader contact surfaces like the palm to distribute load, achieving therapeutic depth without exceeding the tensile threshold of the soft tissue.
Assessment Protocols for the Older Client
In our curriculum, we emphasize that history taking is a critical safety filter. The assessment phase must identify red flags common in this population, particularly regarding medication. Many clients in this age group are on anticoagulant therapy to manage cardiovascular risks. This drastically alters the hemostatic response, meaning even moderate pressure can cause subcutaneous hemorrhaging.
We also visually assess for dermatoporosis – skin that has thinned and lost the structural anchors between the epidermis and dermis. Without these anchors, the shearing forces typical of Swedish massage can cause skin tears. In these cases, we abandon high-friction strokes in favor of static compression or lift-and-hold techniques. Furthermore, we must evaluate for sensory deficits. If a patient has neuropathy, they cannot accurately provide feedback on pressure or heat. In these instances, the therapist must rely exclusively on tissue response rather than verbal cues.
Addressing Mobility Challenges and Joint Stiffness
A primary complaint we encounter is a progressive loss of independence due to restricted range of motion. Addressing these mobility challenges requires a shift from passive stretching to active-assisted mobilization. Static stretching can be detrimental because the stretch reflex is often delayed, and tendon tensile strength is reduced in elderly populations.
Conversely, gentle joint mobilization using small, rhythmic oscillations stimulates the production of synovial fluid. This lubrication is vital for nourishing avascular cartilage. When we observe the kinetic chain of an aging body, we frequently see a posterior pelvic tilt forcing the thoracic spine into hyper-kyphosis. This limits respiratory efficiency. Therefore, our work targets the anterior chest wall to open the rib cage, improving vital capacity alongside posture.
Hemodynamics in Massage Therapy
Hemodynamic stability is a concept rarely taught in basic schools, yet it is vital when working with elderly populations. Orthostatic hypotension, a sudden drop in blood pressure upon standing, is prevalent. During massage therapy, the parasympathetic nervous system is activated, causing vasodilation. If a therapist abruptly ends a session and asks the person to stand, the risk of syncope (fainting) is high.
To mitigate this, we engineer the conclusion of the session to gradually reintroduce sympathetic tone. We end with active movement of the extremities to encourage blood circulation back to the heart. Furthermore, we strictly avoid the “face cradle” if it forces the neck into extension due to a kyphotic upper back. We build a support structure using bolsters to maintain a neutral cervical spine, ensuring vertebral artery flow remains uncompromised.
The Role of Therapy in Pain Management
Discomfort in this demographic involves both tissue damage and neuropathic components. The “no pain, no gain” philosophy is entirely inappropriate. Our goal with therapy is to modulate the nervous system’s perception of distress through the Gate Control Theory. By stimulating mechanoreceptors with smooth, consistent tactile input, we can inhibit the transmission of nociceptive signals.
This approach validates the use of lighter massage techniques as a neurological intervention. We are hacking the nervous system to lower central sensitization. When a patient lives in chronic pain, their nervous system becomes hyper-reactive. Gentle, non-threatening touch teaches the brain that movement does not always equal danger. Additionally, for those living in isolation, the release of oxytocin during a session provides a biochemical counter-weight to the psychological stressors that often exacerbate physical suffering.
Geriatric Care and Health Span
At RSM International Academy, we align our teachings with the concept of “health span”, the number of years a person lives in good health, as opposed to just total life span. Massage therapy plays a crucial role here by preserving movement. Movement is the signal that tells the body to maintain bone density and joint lubrication.
When stiffness limits movement, the body enters a spiral of decay. By reducing pain and restoring passive range of motion, we enable the patient to move more. This movement feeds back into the system, improving circulation and cognitive function. The benefits of this approach extend beyond the physical; we educate the patient on the difference between “hurt” and “harm.” Many older clients avoid movement due to fear of damage. By providing safe, passive motion on the table, we build their confidence to remain active.
The line between massage and rehabilitation blurs significantly in this context. While we do not replace physical therapists, our work prepares the tissue for their interventions. A muscle that is ischemic responds poorly to strengthening. By restoring resting tone, we create a window where strengthening exercises are more effective. This integration is particularly relevant for the treatment of conditions like frozen shoulder, where navigating the balance between inflammation relief and mobilization is critical.
Achieving Clinical Value
The field of gerontology is expanding, and what we know about aging physiology has been refined. We now know that neuroplasticity persists well into late life, meaning proprioceptive training and wellness interventions can improve balance even in advanced age.
For massage therapists, this demographic represents a massive portion of future clientele. Ignoring their specific needs is professional negligence. When we approach the senior body with respect for its history and biology, we support the dignity of independence. We facilitate the ability to move through the world with less restriction. This is the core mission of sports medicine-based massage therapy: to optimize function at every stage of life. The elderly clients we serve are not fragile glass, but complex biological systems that possess a remarkable capacity for restoration when treated with clinical precision.
Anatomy Basics for Sports Massage

Sports Massage for Athletic Conditioning Management
To truly master manual therapy, a therapist must move beyond simple memorization and visualize the three-dimensional relationship between structure and function. I often remind students in RSM's Sports Massage Course that anatomy is not a static subject; it is a dynamic map that changes with every injury and compensation pattern.
When a student understands the musculoskeletal system, massage therapy transforms from routine surface rubbing into a precise clinical intervention. If a therapist cannot visualize the layers beneath their hands, they are guessing. However, when they possess a deep understanding of the body, every stroke becomes a deliberate communication with living tissue, capable of resolving pain and optimizing function.
Why Applied Anatomy is Vital for Effective Massage
Structure cannot be separated from function. Knowing the name of a muscle is less important than understanding how it reacts to pressure. A lack of knowledge leads to vague treatments, whereas precise human anatomy knowledge allows a therapist to navigate with confidence.
Safety is paramount. The body contains vulnerable zones where nerves and arteries are superficial. A therapist who knows their anatomy understands exactly where to apply force and where to back off. Beyond safety, efficacy drives the need for study. A client with shoulder pain may actually be suffering from a rib cage restriction. Without understanding the interconnected nature of the body systems, a therapist might chase symptoms rather than addressing the root cause.
The Skeletal System: The Framework of Movement
Muscles attach to bone; therefore, the skeletal system is the prerequisite for understanding soft tissue. Bones act as levers, and joints serve as fulcrums that allow movement. When teaching palpation, I insist that students first locate bony landmarks. These are the only reliable navigation points on the body.
For instance, scapular position dictates rotator cuff tension. If the scapula is misaligned, the shoulder joint loses its center of rotation. Recognizing the position of these landmarks allows the therapist to assess whether the skeleton is providing a stable base. Furthermore, joint mechanics dictate the limits of massage. Forcing a joint beyond its physiological barrier triggers protective spasms, counteracting the therapy.
The Muscular System: Layers, Origins, and Insertions
The muscular system is the primary target for sports massage, but it is often misunderstood as a uniform layer. In reality, muscles are arranged in complex, overlapping sheets. To treat these structures effectively, a therapist must visualize their origins insertions.
This knowledge reveals the direction of the fibers, which is critical for technique application. Friction must often be applied parallel or perpendicular to the fiber direction to be effective. We must also analyze muscle tone to distinguish between two distinct states:
- Locked Short: The muscle is shortened and tight due to overuse (e.g., tight pecs).
- Locked Long: The muscle is lengthened and taut, straining to counter an opposing force (e.g., strained rhomboids).
Treating a “locked long” muscle with deep pressure often aggravates the issue. This nuance is only possible when one understands muscle anatomy and the physiological state of the tissue.
Understanding Muscle Groups and Functional Chains
In sports, movement is a symphony of coordinated actions involving multiple muscle groups. We refer to these functional connections as kinetic chains. When a link in the chain fails, the load transfers elsewhere. For example, knee pain in runners often originates from weak hip stabilizers.
If I focused solely on the knee, I would fail to resolve the problem. Because muscles connect via fascia, a restriction in the shoulder can theoretically inhibit the opposite hip. Recognizing these patterns allows therapists to think globally while treating locally.
The Nervous System: The Forgotten Component
While we manipulate tissue, we are ultimately communicating with the nervous system. Physiology dictates that muscle tone is regulated by the brain and spinal cord. Often, stiffness is a neurological “alarm” rather than tissue damage.
Aggressive techniques that cause excessive pain can trigger a sympathetic defense response, causing muscles to tighten further. Conversely, our goal is to downregulate the nervous system to prevent guarding. By understanding these neurological reflexes, we can facilitate genuine recovery.
Integrating Body Systems for Clinical Success
The separation of these systems is academic; in the living body, they function as one unit. The skeletal system provides levers, the muscular system provides force, and the nervous system provides control.
At RSM International Academy, we use this integrated understanding to correct asymmetries before they become injuries. When you can visualize the sliding filaments of a muscle fiber and the firing rate of a motor unit, your hands become intelligent tools. This proactive approach is the standard we strive for in performance therapy.
Unlocking the Key Principles of Shiatsu Massage

Deep Shiatsu Massage Course
One of the most frequent corrections I make during practical training in RSM’s Shiatsu Massage Course is when students attempt to address muscle stiffness by increasing force rather than improving their angle. They mistakenly equate intensity with effectiveness. In our sports medicine curriculum, we emphasize that therapeutic change relies on the precision of application, not the magnitude of strength. This distinction forms the foundation of the key principles of shiatsu massage.
Unlike Western modalities that utilize friction and gliding strokes to stimulate venous return, this method operates on a unique biomechanical logic. It is a system of static compression designed to interact directly with the body’s proprioceptors and autonomic nervous system. To master this art, practitioners must move beyond memorizing points and start visualizing the relationship between perpendicular force, tissue resistance, and neurological response. By integrating traditional Japanese wisdom with modern sports science, we transform abstract concepts into clinical tools that reliably treat pain and dysfunction.
The Science of Shiatsu Pressure and Body Mechanics
The primary differentiator of this modality is the application of vertical pressure. For force to transmit effectively into deep musculature without triggering a protective guarding response, it must enter the surface at exactly 90 degrees. If the angle deviates, the force vector splits, creating a shearing action across the skin. This shearing stimulates surface nociceptors, causing the client to intuitively tense up.
Conversely, when pressure is applied perpendicularly, the body accepts the intrusion. The force bypasses superficial defense mechanisms and reaches the deep muscle spindles. This allows the therapist to affect the gamma loop, the feedback system regulating muscle tone. By compressing these fibers directly, we reset their resting tension. Consequently, a smaller therapist using correct alignment can effect greater change than a stronger therapist pushing at an oblique angle.
This principle extends to the therapist’s own biomechanics. We do not use muscular effort to push. Instead, we stack our bones – thumb, wrist, elbow, and shoulder – in a straight line. This creates a solid column that transfers the weight of the core (Hara) directly into the client. This protects the therapist’s joints while delivering a stable, grounding sensation that promotes trust and safety.
Achieving Relaxation Through Sustained Compression
Once the correct depth and angle are achieved, the next variable is duration. While standard massage protocols often favor rhythmic, continuous movement, shiatsu relies on the power of the “stop.” This principle of stationary, sustained compression is rooted in the viscoelastic properties of connective tissue.
Fascia exhibits a behavior known as “creep.” When a constant load is applied, the tissue slowly deforms as water content redistributes and collagen fibers align with the stress. Quick compressions stimulate Pacinian corpuscles, which detect vibration but do not lower tone. In contrast, sustained static pressure engages Ruffini endings. These slow-adapting receptors respond to constant stretch by signaling a global inhibition of sympathetic activity.
This physiological shift is what we define as true relaxation. It is not merely a subjective feeling of comfort but the dominance of the parasympathetic nervous system over the sympathetic “fight or flight” response. Chronic stress and sports injuries often trap clients in a sympathetic state, hindering tissue repair. By stimulating the vagus nerve through deep, static pressure, shiatsu massage lowers heart rate and facilitates the recovery processes essential for physical health.
Diagnostic Touch and Energy Balance
A common misconception is that this therapy is purely energetic. However, when we overlay meridian lines with anatomical maps, we see they often trace deep fascial chains and neurovascular bundles. Treating these lines restores mechanical glide between tissues. To do this effectively, we use a two-hand technique: the “Mother Hand” (stationary support) and the “Child Hand” (active worker).
This connection creates a closed kinetic chain, allowing the therapist to listen to the tissue’s reaction. It also facilitates the diagnosis of “Kyo” and “Jitsu” states, which is central to our clinical approach.
- Jitsu (Excess): Areas that feel hard, resistant, and often painful. This is usually where the client complains of symptoms.
- Kyo (Deficiency): Areas that feel empty, cold, or weak. These spots lack resilience and often represent the root cause of the dysfunction.
Novice therapists often attack the Jitsu tension. However, Jitsu is frequently a compensatory reaction to a Kyo weakness elsewhere. For example, a tight lower back (Jitsu) may be compensating for weak glutes (Kyo). By nourishing the Kyo area with sustained, supportive techniques, we restore its load-bearing capacity. As a result, the Jitsu area releases naturally because it no longer needs to overwork. This diagnostic logic ensures we treat the cause rather than just the symptom, restoring functional balance to the kinetic chain.
Integrating Shiatsu Massage into Sports Medicine
At RSM, we view shiatsu bodywork as a vital component of athletic recovery. The concept of “energy” or Qi flow translates clinically to the unobstructed circulation of blood, lymph, and nerve impulses. When working with athletes, this improved flow flushes metabolic waste from ischemic tissue and reduces recovery time.
Furthermore, the emphasis on the Hara teaches clients to move from their center. As therapists, we model this stability. By generating force from our core, we subtly re-educate the client’s proprioception. Whether treating an elite runner or a desk worker, the goal remains the same: to create a physiological environment where the body can heal itself.
By adhering to the principles of perpendicularity, stationarity, and diagnostic assessment, we elevate wellness practices to the level of clinical excellence. We do not force the tissue; we provide the stable fulcrum against which the body reorganizes. This precise, evidence-based approach is what makes shiatsu an indispensable tool in modern sports medicine.
The Importance of Anatomy in Massage Education

Sports medicine massage course
I see a distinct dividing line between a standard practitioner and a true clinical specialist. It’s a line which is drawn by the depth of their understanding of the human frame. Many students arrive at our massage school in Thailand with a passion for healing, believing that intuition alone guides the hands. However, intuition without a map is merely guessing. When a therapist relies on memorized sequences rather than a concrete mental image of the structures beneath the skin, the treatment hits a ceiling. Conversely, a profound grasp of structure transforms a routine session into a targeted medical intervention.
Elevating Massage Therapy Through Science
The shift from relaxation to sports medicine-based massage therapy requires a fundamental change in mindset. We are not simply rubbing skin; we are manipulating a complex biological machine. When massage therapy is applied with scientific precision, it influences fluid dynamics, alters fascial tension, and resets neuromuscular tone. This level of efficacy is impossible without a rigorous study of the underlying architecture.
Consider a client presenting with chronic lower back pain. A superficial approach might suggest rubbing the erector spinae because that is where the symptoms manifest. However, a practitioner grounded in sports medicine recognizes that the lumbar spine is often a victim of hip immobility. The tightness in the lower back is a compensatory reaction to a restricted psoas major pulling on the lumbar vertebrae. Consequently, the massage therapy treatment plan shifts. We stop chasing the pain and start treating the dysfunction. This logical progression is the core value of our school and the foundation of effective massage.
Why Anatomy Knowledge Separates the Pros
Acquiring deep anatomy knowledge is not about memorizing Latin names; it is about visualizing depth and texture in three dimensions. When I teach palpation, I emphasize that every layer feels distinct. Muscle tissue has a specific grain and density. Connective tissue, such as fascia and tendons, feels more fibrous and unyielding. Nervous tissue is cord-like and highly sensitive.
Without precise anatomy knowledge, a therapist cannot differentiate between a trigger point and an inflamed bursa. Misidentifying these structures leads to improper technique application. Pressing hard on an inflamed bursa because it “feels tight” will only aggravate the inflammation. In contrast, knowing the exact location of the subacromial bursa allows the therapist to mobilize the surrounding muscles without compressing the sensitive fluid sac.
This distinction is critical for safety. The anterior neck contains the carotid artery and the vagus nerve. A therapist lacking human anatomy training might apply deep pressure here, inadvertently compressing the carotid sinus. Safety is the first priority. A massage applied without this awareness is not just ineffective; it is dangerous.
Decoding the Body for Better Results
The body functions as a tensegrity structure. A failure in one area ripples through the entire system. At RSM, we view the body not as a collection of isolated parts but as an integrated kinetic chain.
For instance, plantar fasciitis often presents as heel pain. However, investigating the body structurally often reveals that tight calf muscles are limiting ankle dorsiflexion, forcing the plantar fascia to overstretch. Going further up the chain, weak glutes may cause internal femoral rotation, collapsing the arch. By treating the calf and activating the glutes, we alleviate the tension downstream. Pain is rarely where the problem lives; it is merely where the system is failing to handle the load.
Integrating Physiology Knowledge
While anatomy provides the map, physiology knowledge explains the traffic flow. It is not enough to know where a muscle attaches; we must understand how the nervous system controls it. Massage is, in essence, a conversation with the nervous system.
We utilize concepts like Reciprocal Inhibition to manipulate muscle tone. If a client has a spastic hamstring, fighting it with deep pressure often triggers a protective stretch reflex. Instead, applying physiology knowledge, we know that contracting the opposing quadriceps forces the nervous system to relax the hamstring. This physiological hack achieves release without brutality.
Essential Anatomy in Practice
To illustrate the practical application of this philosophy, here are specific areas where anatomical precision dictates the success of the massage:
- The Suboccipital Triangle: Many tension headaches originate here. Precise palpation of the Rectus Capitis Posterior Minor, which bridges to the dura mater, can instantly relieve symptoms.
- The Psoas Major: Accessing this deep stabilizer requires intimate knowledge of the abdominal aorta and inguinal ligament to avoid injury.
- The Piriformis: Differentiating between piriformis syndrome and true lumbar radiculopathy requires specific provocation tests that rely entirely on anatomy.
- The Tarsal Tunnel: Medial ankle pain is often nerve compression, not a sprain. Knowledge of the flexor retinaculum allows the therapist to decompress the nerve rather than irritating it.
The Impact on Therapists
For therapists, essential anatomy is the ultimate safeguard against career-ending injuries. Many massage therapists burn out due to wrist pain caused by poor biomechanics. When therapists understand the leverage points of the skeleton, they learn to stack their joints and use their body weight rather than hand strength.
Targeting specific layers reduces the effort required. When you know exactly where the border of the scapula is, you can hook your fingers under the rhomboids with minimal force. You stop fighting the tissues and start working with natural planes.
In my experience, the moment a student truly grasps the connectivity of the muscular system is the moment they stop doing “routines” and start practicing therapy. That confidence is palpable. Therefore, for any aspiring therapist, the directive is clear: Go back to the texts. The power of your touch is directly proportional to the clarity of your anatomical understanding. Without it, you are merely skimming the surface. With it, you facilitate true recovery.
Clinical Approaches to Myofascial Release for Back Pain

Dynamic Myofascial Release Course
I often see patients, and students in our Myofascial Release Course, puzzled by the same recurring issue: back pain that refuses to go away. They treat the muscles, adjust the spine, and rest, yet the restriction returns. This cycle persists because standard treatments often ignore the structural glue holding the body together: the fascia. To truly resolve these chronic issues, we must look beyond the vertebrae and understand the mechanics of myofascial release.
The Mechanics of Myofascial Release
Fascia is not merely passive wrapping; it is a fluid-dependent system. In our curriculum, we teach the concept of thixotropy. Under healthy conditions, the ground substance of the fascia acts as a lubricant, allowing muscles to slide efficiently. However, trauma, inflammation, or immobility causes this substance to turn from a fluid state into a viscous, gel-like solid.
This rigid gel binds muscle fibers together, creating pressure on pain-sensitive structures. When we apply sustained myofascial release, we are adding mechanical energy to the system. This energy creates heat and piezoelectricity, signaling the tissue to reorganize and the ground substance to return to its fluid state. Consequently, the restriction melts, and the trapped nerve endings are freed.
This distinguishes myofascial release from standard massage. While massage often uses rhythmic strokes to flush fluids and relax muscles, release techniques engage the varying barriers of the fascial tissues. We do not force the barrier; we wait for the body to yield.
Restoring the Hydraulic Amplifier
A critical concept we emphasize is the “Hydraulic Amplifier” mechanism of the Thoracolumbar Fascia (TLF). In a healthy back, contracting the paraspinal muscles expands them against the fascial sheath, creating intra-abdominal pressure that stabilizes the spine.
However, if the myofascial layers are fibrosed, the sheath cannot expand. The hydraulic mechanism fails. As a result, the load transfers directly to the discs and facet joints, leading to wear and pain. Effective treatment must restore elasticity to the TLF. By freeing these myofascial tissues, we allow the muscles to expand correctly, reinstating the hydraulic support system that protects the spine.
Identifying Myofascial Pain Syndromes
Myofascial pain rarely originates exactly where it hurts. The body is a tensegrity structure; a restriction in one area creates tension in another. A prime example is the Posterior Oblique Sling, which connects the Gluteus Maximus to the opposite Latissimus Dorsi via the Thoracolumbar Fascia.
If a patient has a weak left glute, the right Latissimus Dorsi overcompensates, tightening the fascia across the lower back. The patient feels pain in the lumbar region, but the root cause is a myofascial imbalance in the sling. Treating the back alone provides only temporary relief. In contrast, addressing the entire sling restores function and eliminates the mechanical stress causing the pain.
Differentiating Myofascial Release from Massage
It is vital to distinguish the modality. In massage, the goal is often relaxation, using oil to glide over the skin. Myofascial release requires a high coefficient of friction. We do not slide; we shear.
We anchor the skin and apply tangential force to engage the underlying connective tissue. We hold this pressure for 90 to 120 seconds. This approach addresses the viscoelastic nature of the fascia, ensuring plastic (semi-permanent) elongation rather than elastic (temporary) stretching. This is why release therapy is often more effective for chronic pain management than techniques that only address muscle tone.
The Role of Myofascial Release Therapy in Spinal Health
The Paraspinal Retinacular Sheath (PRS) is a deep layer of fascia separating the spinal muscles from the Quadratus Lumborum (QL). In many sufferers, this sheath adheres to the muscles, preventing independent movement.
Myofascial Release therapy here is profound. By manually separating the erector spinae from the QL, we reduce friction and break the inflammatory cycle. This decoupling allows the lumbar vertebrae to move without dragging the rib cage and pelvis, which is essential for pain-free motion.
Precision is the hallmark of the RSM method. We do not guess. If fascia is restricted in a superior-medial direction, simply pushing down will trigger a defense response. We must engage the tissue in the exact vector of the restriction. This precision minimizes discomfort during treatment and maximizes the relief felt afterwards.
Integrating Myofascial Release for Long-Term Results
Ultimately, myofascial release acts as a reset button. It clears restrictions and reduces pain signals. However, if the patient returns to poor movement patterns, the fascia will reorganize back into the dysfunctional pattern. Rehabilitation must immediately follow the release.
At our academy, we advocate a structured integration protocol:
- Release: Use myofascial release to melt adhesions and restore hydration to the tissue.
- Mobilize: Perform active mobility drills to utilize the new range of motion.
- Activate: Isolate weak muscles (often the glutes) that forced the back to compensate.
- Integrate: Perform functional movements to cement the new pattern into the nervous system.
By following this protocol, we transition from passive treatment to active pain management. We stop treating the symptom and start correcting the biomechanical root cause. Myofascial release bridges the gap between structure and function, offering a pathway out of the cycle of pain and back to resilient movement.
