
RSM Blog: Sports Medicine and Massage Insights
The Importance of Client Assessment Skills for Elite Therapists
Sports Medicine Postural Assessment
A major distinction between a spa masseur and a clinical sports therapist lies in their analytical capability. Practitioners who skip detailed evaluation are essentially guessing. Conversely, therapists who master the art of observation can identify the root cause of dysfunction often before they even touch the client.
In RSM's Remedial Massage Course we emphasize that client assessment is not a static checklist; it is a dynamic investigation. When a client presents with lower back pain, a novice might immediately massage the lumbar erectors. However, an expert understands that this pain is often a compensatory price paid for hip stiffness or thoracic immobility. Without a structured process of investigation, treatment becomes symptomatic rather than corrective. As a result, the pain returns, and the client’s faith in the therapy weakens.
The Role of the Client in the Intake Phase
The foundation of any clinical interaction begins with the Subjective Assessment. This phase serves a dual purpose: gathering data and establishing trust. When a client shares their medical history and lifestyle habits, they provide the necessary context to construct a hypothesis.
We must listen for what is not said. A client might mention occasional knee pain while seeking help for a shoulder issue. To a sports medicine practitioner, this could indicate a cross-body pattern dysfunction. If we fail to ask the right questions, we miss the Red Flags that might contraindicate massage, such as deep vein thrombosis.
Developing Effective Communication Skills
High-level communication skills involve translating complex physiological concepts into language the client understands. If I explain that “femoral rotation is pressuring your knee” rather than using complex medical jargon, the client grasps the mechanism.
This clarity fosters compliance. When a client understands the “why” behind their pain, they become active participants in their recovery rather than passive recipients of treatment. This partnership is the hallmark of modern sports medicine.
Core Assessment Methods and Strategies
Once subjective data is collected, we move to Objective Assessment. Among the various assessment methods, Static Postural Analysis is the first step. We observe the client standing, looking for deviations from the midline like head-forward posture or hip discrepancies.
However, static posture is limited. Human bodies are designed for motion. Consequently, a client might appear aligned while standing but exhibit dysfunction when moving. This necessitates Dynamic Postural Assessment. In our curriculum, we use tools like the BOSU ball to test neuromuscular integration. We watch for “tells”, such as ankle pronation or knee valgus, that reveal the integrity of the kinetic chain. These dynamic tests expose weaknesses that a massage table hides.
Selecting the Right Assessment Tools
To quantify our findings, we must employ precise assessment tools. We cannot manage what we cannot measure.
- Goniometers: Measuring Range of Motion (ROM) establishes a baseline to track progress.
- Palpation: This is our primary scanner. We feel for hypertonicity and temperature changes, distinguishing between acute inflammation and chronic ischemia.
- Orthopaedic Tests: Specific maneuvers, such as the Empty Can test or Anterior Drawer test, stress particular tissues to isolate the injury.
Using these instruments allows us to differentiate between tissues. Is the limitation caused by a short muscle or a capsular restriction? The answer dictates the treatment.
Interpreting the Client’s Physical Data
Data collection is useless without accurate interpretation. We must synthesize findings from history taking and ROM tests to form a cohesive picture.
Consider a runner with plantar fasciitis. Observation might reveal high arches, while ROM testing shows limited ankle dorsiflexion. Palpation may confirm extreme calf tightness. Connecting these dots reveals that the plantar fascia is being overstressed because the calf muscles prevent proper ankle movement. Therefore, treating the foot alone is insufficient; we must release the calf. This level of deduction is only possible through rigorous skills in assessment.
The Responsibility of the Trainer and Therapist
Whether you are a sports massage therapist or a personal trainer, your duty of care is paramount. A trainer who loads a client with heavy squats without assessing hip mobility invites injury. Similarly, a therapist who performs deep tissue manipulation on a neck without screening for vertebral artery insufficiency risks severe harm.
Assessment is our safety net. It protects the client from injury and the practitioner from liability. At RSM, we teach that if you cannot replicate a symptom or identify a mechanical fault, you should treat with caution. If a client presents with symptoms that do not fit a mechanical pattern, for example unrelenting night pain, these are red flags requiring medical referral. Knowing when not to treat is as important as knowing how to treat.
Client Assessment as a Continuous Cycle
Assessment is not a one-time event; it is a continuous loop.
- Pre-treatment: Establishes the plan.
- During treatment: Palpation provides real-time feedback. If a muscle spasms, the nervous system is guarding, indicating we must adjust our pressure.
- Post-treatment: We re-test the markers. If the client had limited neck rotation, has it improved?
This “Test-Treat-Retest” model provides immediate validation. It proves to the client that the therapy is working. If there is no change, it forces us to re-evaluate our hypothesis. This honest audit drives professional growth.
Anatomy of a Misdiagnosis
To illustrate the danger of skipping assessment, consider “Sciatica.” This term is often used loosely by clients to describe posterior leg pain.
True sciatica is often a lumbar spine issue. However, Piriformis Syndrome mimics these symptoms perfectly when the piriformis muscle entraps the sciatic nerve. If a therapist assumes the issue is spinal, they might avoid the gluteal region. Conversely, treating it as a hamstring strain misses the neural component.
Through specific orthopedic tests like the Straight Leg Raise, we can differentiate between a lumbar root issue and a peripheral entrapment. The correct functional diagnosis determines the outcome.
Integrating Assessment for Professional Success
For the busy practitioner, the objection is often time. “I don’t want to waste 15 minutes talking.” This is a false economy. Spending 10 minutes on clinical assessment ensures the remaining 50 minutes are effective.
Efficient assessment does not need to be lengthy. With practice, a visual scan takes seconds. Palpation happens simultaneously with warm-up strokes. We teach our students to “assess as you go.” Every stroke provides information. The skills assessment of a therapist is defined by their ability to treat and evaluate simultaneously.
Furthermore, explaining findings to a client demonstrates expertise. If you can tell a client, “Your shoulder pain is linked to a restriction in your opposite hip,” you validate their pain and build loyalty.
Our Assessment Philosophy
Mastering these protocols requires dedication. But the reward is the ability to facilitate true healing. At RSM International Academy, we believe that the power of the hands is limited without the guidance of the mind. By prioritizing rigorous, comprehensive assessment, we ensure that every treatment is safe, specific, and successful.
Whether you are dealing with an Olympian or a weekend warrior, the principle remains: Assess, don’t guess. The body holds the answers; we simply need the skills to read them.
Exploring Fascia Anatomy and Function in Manual Therapy

Myofascial Anatomy for Sports Massage
In traditional textbooks, the “red” muscle tissue gets all the attention, while the “white” connective tissue is often dissected away and discarded to reveal the “more important” structures underneath. However, this reductionist view fails to capture the reality of human movement. Students of RSM's Dynamic Myofascial Release Course learn that the body is not a collection of parts but a unified, tension-dependent network. To truly treat pain and dysfunction, we must shift our focus to the architecture that holds it all together.
Defining the Fascial System Beyond Simple Wrapping
Many therapists mistakenly define fascia as merely the “packaging material” of the body. They see it as the passive casing that separates the biceps from the triceps or the skin from the muscle. While it certainly performs this separating function, this definition is woefully incomplete. Fascia is better understood as a continuous, three-dimensional signaling network that permeates every corner of the human form. It wraps around individual muscle fibers, bundles them into fascicles, encases the entire muscle belly, and then continues to become tendons, ligaments, and even the matrix of the bone itself.
Consequently, no muscle functions in isolation. When the quadriceps contracts, it does not just pull on the tibial tuberosity; it transmits tension laterally into the fascial envelope of the thigh and superiorly into the hip. This concept forms the basis of bio-tensegrity (biological tension-integrity). In a tensegrity structure, rigid components (bones) do not stack on top of each other like a column of bricks. Instead, they float inside a continuous tension network of soft tissue. This arrangement allows the body to distribute impact forces globally rather than locally. When an athlete lands a jump, the shock is not absorbed solely by the ankle joint; it is dispersed instantly through the entire fascial system.
The Microscopic and Macroscopic Structure of Fascia
To understand how to treat this tissue effectively, we must look at its composition. Fascia is comprised of cells and the Extracellular Matrix (ECM). The primary cells, fibroblasts, are the architects responsible for synthesizing the fibers and ground substance that make up the ECM. Interestingly, fibroblasts are mechanosensitive. This means they respond to physical strain, such as exercise or manual therapy, by remodeling the tissue architecture. If a body part remains stationary for too long, fibroblasts lay down more collagen in a disorganized manner, creating stiffness. Conversely, regular, multi-directional movement stimulates them to align collagen fibers along the lines of stress, creating resilience.
The ECM itself consists of two main elements: the fibrous network and the ground substance. The fibers are primarily collagen (for strength) and elastin (for recoil). The ground substance, however, is often the game-changer in manual therapy. It is a gel-like medium rich in glycosaminoglycans (GAGs), specifically hyaluronic acid, which binds water to create a lubricant. In a healthy state, this fluid environment allows fascial layers to glide effortlessly over one another.
However, when tissue becomes dehydrated or inflamed, the hyaluronic acid becomes sticky and viscous. This creates densification, where the sliding surfaces adhere to one another. As a result, the muscles underneath cannot contract or lengthen efficiently. This microscopic “glue” is often what we feel as a “knot” or restriction. It is not necessarily a muscle spasm; it is often a failure of the fascial lubrication system.
How Fascia Connects Muscles into Functional Chains
The continuity of fascia means that force transmission is not linear. Research indicates that a significant percentage of the force generated by a muscle fiber is not transmitted directly to the tendon but is instead dispersed laterally into the surrounding fascial sheets. This phenomenon, known as epimuscular force transmission, links parallel muscles together.
This leads to the concept of myofascial chains or meridians. A restriction in the plantar fascia of the foot can transmit tension up the posterior chain, affecting the hamstrings, the sacrotuberous ligament, and eventually the suboccipital region at the base of the skull. Therefore, treating a client’s tension headache might require addressing tight structures in their calves. If we only treat the site of pain, we often miss the mechanical cause.
This interconnectedness explains why localized stretching is sometimes ineffective. If the fascial suit is tight globally, stretching one isolated section is like trying to pull slack out of a tightly fitted wetsuit; the restriction elsewhere simply pulls back. Effective therapy requires assessing the entire kinetic chain to identify where the “fabric” is bunched or stuck.
Clinical Implications of Fascia Lata and Lateral Stability
A prime example of fascia acting as a dynamic stabilizer is the fascia lata. This deep, dense sheath encases the muscles of the thigh like a high-compression stocking. Its structural integrity is critical for venous return, as it limits the outward expansion of the contracting muscles, forcing blood up against gravity.
Laterally, the fascia lata thickens significantly to form the iliotibial tract (or IT band). Many novice therapists view the IT band as a nuisance – a rigid strap causing “runner’s knee” – that needs to be pummeled into submission. This is a misunderstanding of its function. The IT band is an anchor. It receives insertions from both the tensor fascia latae (TFL) and the gluteus maximus.
Because of these connections, the fascia lata acts as a lateral stabilizer for the knee, especially during the single-leg stance phase of running or walking. If the gluteus maximus is weak or inhibited, the TFL often compensates by contracting excessively. This tension pulls the fascia lata taut, potentially compressing the distal fat pad at the knee or creating friction.
However, simply “rolling out” the IT band is rarely the answer. The IT band itself is incredibly strong – studies suggest it has the tensile strength of soft steel – and it cannot be mechanically lengthened by a foam roller. Instead, the goal of therapy should be to restore the sliding capacity between the fascia lata and the underlying vastus lateralis, and to normalize the tone of the attached muscles (the gluteals and TFL). By restoring the glide, we reduce the friction and drag that causes the pain.
The Role of Fascial Tissue in Proprioception and Pain
For decades, we believed that muscles and joints were the primary sources of proprioception (the body’s sense of position in space). We now know that the fascial network is one of the body’s richest sensory organs. It is densely innervated with mechanoreceptors, including Ruffini endings, Pacinian corpuscles, and free nerve endings.
Ruffini endings are particularly interesting for manual therapists because they respond to slow, sustained tangential pressure: the exact type of shearing force applied during myofascial release. When these receptors are stimulated, they lower the tone of the sympathetic nervous system, inducing global relaxation. This explains why slow, deep fascial work often feels more relaxing to a client than rapid, percussive massage.
Furthermore, fascia is a major source of pain. Many conditions diagnosed as “muscle strain” or “tendonitis” are actually pathologies of the fascial tissue. The densification of the deep fascia can entrap free nerve endings, creating sharp, localized pain. In other cases, the thickening of the tissue alters the input to the nervous system, confusing the brain’s map of the body. This leads to clumsy movement patterns and further injury. By refining the tactile acuity of the fascial system, we do not just reduce pain; we improve the athlete’s movement efficiency and coordination.
Applying These Concepts at RSM International Academy
At RSM International Academy, we integrate these anatomical realities into every practical technique we teach. We emphasize that you cannot force fascia to release. Since it is a non-Newtonian fluid system (the ground substance changes viscosity under stress), aggressive force often causes the tissue to harden in defense via a phenomenon known as shear thickening.
Instead, we teach students to engage the fascial barrier with patience. We use specific shearing angles to stimulate the Ruffini endings and encourage the re-hydration of the ground substance. The goal is to melt the “glue” rather than tear the fibers. When I observe students working, I look for “sink and glide” rather than “push and shove.”
We also emphasize the importance of active movement. Passive treatment alone is rarely enough to remodel collagen architecture. Following the manual release, we must load the tissue through its full range of motion to signal the fibroblasts to lay down new collagen in a functional alignment. This combination of hands-on release and movement re-education is the cornerstone of modern sports medicine.
Understanding anatomy in this way transforms a therapist from a technician into a clinician. It allows us to solve complex pain puzzles rather than just chasing symptoms. When we respect the continuity of the body and the intelligence of the fascial system, we unlock a higher level of therapeutic potential.
Understanding the Benefits of Group Massage Practice

Deep Tissue Massage Course for posture correction
In my experience working with elite sports teams and professional athletes, I've found it important to consider the physiological influence of the social environment. When we shift our perspective from individual isolation to a collective setting, the mechanisms of recovery change. The shared environment triggers neurological pathways that can actually amplify the effects of manual therapy.
At RSM's Massage School in Chiang Mai, Thailand, we emphasize that a therapist must be adaptable. While privacy is essential for specific clinical interventions, contexts like training camps or corporate offices utilize the collective atmosphere as a catalyst for recovery. By understanding how social dynamics influence the autonomic nervous system, we better appreciate why treating multiple individuals in a shared space is a valid therapeutic strategy.
The Physiology of Shared Wellness
The efficacy of manual therapy relies heavily on the recipient’s state of autonomic arousal. When an individual receives treatment in a safe, communal environment, a phenomenon known as co-regulation often occurs. This biological process allows nervous systems to synchronize, promoting a collective shift from sympathetic fight-or-flight states toward parasympathetic rest-and-digest states.
In a solitary session, the client must self-regulate to reach a state of deep relaxation. In a group setting, however, the presence of others who are also entering a relaxed state accelerates this process. This is evident in mammals, who rely on the herd for safety. When a client perceives that their peers are safe, their amygdala lowers its guard more rapidly. This leads to a more efficient downregulation of stress hormones. Consequently, the mechanical work performed by the therapist encounters less neuromuscular resistance.
Social Buffering Mechanisms
Research describes this as “social buffering,” where a supportive social network mitigates the physiological response to stress. In a massage context, the shared experience creates a feedback loop. One person’s visible calm signals safety to others. By harnessing this dynamic, we achieve outcomes in stress management that might take longer to achieve in isolation.
Enhancing Team Dynamics Through Manual Therapy
In sports medicine, the locker room is a hub of activity. Integrating massage therapy here does more than treat injuries; it reinforces the cohesion of the team.
When athletes receive treatment side-by-side, it normalizes the culture of recovery. It transforms maintenance care into a standard component of training. This shared vulnerability fosters trust. An athlete seeing their teammate prioritizing recovery is more likely to adopt similar habits. Furthermore, the release of oxytocin during positive physical touch strengthens the bonding group dynamic. The massage sessions become a ritual of collective care.
The Role of Corporate Wellness Programs
These principles transfer effectively to the corporate sector. Modern work environments often induce chronic sedentary posture and sustained sympathetic arousal. Implementing corporate wellness initiatives utilizing on-site manual therapy addresses these issues directly.
A “massage collective” approach disrupts the stress pattern without requiring employees to leave the premises. The impact of stress reduction in these settings is measurable. When employees observe colleagues taking time for self-care, the culture shifts. The brief respite resets resting muscle tone, and because this happens within the workplace, the benefits ripple outward, improving morale across the department.
Optimizing the Massage Experience
Delivering high-quality care in a shared environment requires specific adjustments. The massage experience must be curated to ensure privacy while maintaining the advantages of the open setting.
- Acoustic Management: Ambient music acts as a sonic curtain, providing privacy for relaxation.
- Visual Screening: Portable screens allow clients to feel part of the group without feeling exposed.
- Synchronization: In scenarios involving simultaneous massages, practitioners must coordinate movements to maintain a cohesive atmosphere.
The Educational Advantage at RSM
At RSM International Academy, our students train in a group environment that mirrors professional practice. By rotating partners in a communal space, students learn to focus in distracting environments; an essential skill for sports coverage.
This format accelerates learning. Students benefit from the shared experience of observing different body types and tissue responses simultaneously. Ultimately, the ability to facilitate a social connection through therapeutic touch distinguishes a skilled practitioner. Whether working with a football club or clients in a wellness retreat, the therapist orchestrates an interaction between biology and sociology. By integrating the science of co-regulation with advanced techniques, we move beyond fixing broken parts and start nurturing resilient, connected communities.
Deep Tissue Massage for Athletes: Muscle Recovery & Performance

USA Paralympic National team coach chose RSM
Therapists too often view pressure as the primary variable in effective treatment, believing that to access deeper layers, one must simply apply more force. While teaching the Deep Tissue Massage Course at RSM International Academy, I consistently emphasize that the magnitude of force is secondary to the angle of application and neural receptivity. When working with high-level competitors, this distinction is critical. Digging an elbow into a hypertonic quadricep without preparing the superficial fascia triggers a protective guarding mechanism, defeating the purpose of the therapy.
To truly master bodywork for a high-performance clientele, we must visualize the three-dimensional relationship between neural input, fascial restrictions, and muscular compliance.
The Mechanics of Deep Tissue Massage on Muscle Recovery
Training breaks down muscle fibers and the body repairs them, leading to strength. However, without intervention, this cycle creates adhesions and reduces the sliding potential between tissue layers. A generic massage might flush superficial fluids, but it rarely corrects the structural binding deep within the muscle belly.
Deep tissue massage targets these specific sub-layers. By slowing the stroke and engaging the connective tissue hook, a therapist separates stuck fibers. This restores the muscle’s ability to lengthen fully. A muscle that cannot lengthen cannot contract with maximum force. Therefore, stiffness is a performance inhibitor.
Additionally, hypertonic muscles compress lymph vessels, creating a bottleneck for metabolic waste. Deep tissue techniques mechanically pump fluid through the tissue. By creating positive pressure followed by negative pressure, the therapist acts as an external pump. This accelerates the removal of lactate and brings oxygenated blood to ischemic areas, which is vital for cellular repair.
Breaking Down Scar Tissue and Adhesions
Micro-tearing is a natural result of heavy resistance training. As the body heals, it lays down collagen. Ideally, these fibers align parallel to the muscle fibers. In reality, they often form a disorganized mesh known as scar tissue or adhesions.
These adhesions bind distinct muscle fascicles together. If the lateral head of the gastrocnemius adheres to the soleus, the entire posterior chain functions inefficiently. Deep tissue massage utilizes cross-fiber friction to physically break down these adhesions. The pressure creates a shearing force that disrupts disorganized collagen bonds. Once broken, the body remodels the tissue in alignment with lines of stress, restoring functional elasticity.
Differentiating Sports Massage from Deep Tissue Therapy
There is often confusion regarding terminology. Clients frequently ask for “sports massage” when they need specific deep tissue work. While there is overlap, the clinical intent differs.
Sports massage is an umbrella term encompassing techniques tailored to an athlete’s schedule, including pre-event stimulus and post-event flushing. In contrast, deep tissue massage is a technique-specific modality defined by the depth of the layer engaged. It is almost exclusively a maintenance or rehabilitation tool. You would rarely perform deep tissue work immediately before an event because it temporarily reduces muscle tone.
At RSM, we teach that deep tissue is a tool within the sports massage toolkit. An effective session integrates general warming techniques with focused deep tissue protocols to address specific restrictions.
Addressing Sports Injuries Through Targeted Tissue Manipulation
When an injury occurs, muscles surrounding the site tighten to splint the area. While necessary acutely, chronic splinting leads to compensatory patterns. For example, a mild ankle sprain causes peroneal muscles to tighten. If this tension persists, it limits dorsiflexion. Consequently, the knee absorbs more force, potentially leading to patellar tendonitis.
Deep tissue therapy interrupts this chain. By releasing chronic tension in the peroneals, the therapist restores ankle mobility. This prevents the compensatory load from traveling up the kinetic chain.
Specific applications include:
- Tendinopathies: Releasing the muscle belly reduces tension on the tendon attachment.
- Muscle Strains: Deep work prevents the formation of thick scar tissue at the tear site.
- IT Band Syndrome: Releasing the tensor fasciae latae (TFL) relieves friction causing pain.
The Role of Connective Tissue in Athletic Performance
Anatomy textbooks depict muscles as separate entities, but everything is connected by fascia. Deep tissue massage is frequently more about this connective tissue than the muscle itself.
Athletes rely on the “stretch-shortening cycle” to generate power. Connective tissue provides a significant portion of this elastic energy. If the fascia is rigid, the spring mechanism fails. The athlete must then rely entirely on metabolic muscular contraction, which is less efficient. By keeping the connective tissue hydrated and mobile through slow, melting deep tissue strokes, we optimize this elastic potential.
Integrating Deep Tissue Into Training Cycles
Timing is everything. A therapist must understand periodization to avoid detrimental effects.
Pre-Event: Deep tissue massage is generally contraindicated within 48 hours of competition. Deep work lowers muscle tonus. A sprinter needs high tonus to explode off the line. Relaxing that spring creates a disconnect between the brain and muscle reaction time.
Post-Event: Immediately after an event, the focus is on fluid flushing. The tissue is often micro-traumatized. Aggressive deep tissue work can cause further damage. It is better to wait 24 to 48 hours before engaging deeper layers.
Maintenance Phase: This is the ideal time for deep tissue therapy. Regular sessions during training blocks prevent tension accumulation, allowing the athlete to train harder and recover faster.
Common Misconceptions About Deep Tissue for Athletes
Misconception 1: It Must Hurt to Work.
While some discomfort is inherent in separating adhered tissues, agony is counterproductive. If a client clenches their teeth, the muscle contracts. You cannot release a contracting muscle. The most effective techniques feel intense but relieve pain rather than cause trauma.
Misconception 2: Deeper is Always Better.
Sometimes the restriction is superficial. If the superficial fascia is tight, diving for the deepest layer is ineffective. You must address the layers in order.
Clinical Application
When I observe students in the clinic, the ones who achieve the best results are those who listen to the tactile feedback from the tissue. Deep tissue massage is a powerful intervention that facilitates muscle recovery, breaks down scar tissue, and optimizes performance. However, it must be applied with intelligence.
For the athlete, incorporating this therapy is an investment in longevity. It acts as an alignment check, identifying problems before they become injuries. By prioritizing tissue health, athletes ensure their bodies remain capable of meeting the rigorous demands of their sport, season after season.
Essential Anatomy Knowledge for Massage Therapy in Sports Medicine

Massage training with functional anatomy
Moving Beyond Basic Memorization
To see the study of anatomy merely as a prerequisite for passing a licensing exam overlooks its critical role in solving complex pain patterns. While teaching RSM's Remedial Massage Course, students learn that it is not enough to be able to recite the origins and insertions of muscles. Standard education often presents the human form as a collection of isolated parts rather than an interconnected system. We focus on explaining the sources of the dysfunction, so that students can learn to recognize the true source of a client's chronic pain.
True clinical effectiveness requires a shift in perspective. To truly master the craft, a practitioner must visualize the three-dimensional relationship between bone, muscle, fascia, and nerve. Memorizing attachment points is only the beginning. The real skill lies in interpreting how those points influence leverage and joint compression during movement. Without this depth of understanding, a massage treatment remains superficial, offering temporary relief but failing to correct the underlying mechanical faults.
Integrating Physiology with Structural Analysis
While structural anatomy provides the map, physiology provides the traffic rules. It is impossible to treat tissue effectively without respecting the nervous system that controls it. In our school, we emphasize that a hypertonic muscle is rarely tight by accident; it is often a neurological response governed by muscle spindle cells to prevent joint instability.
If a student applies aggressive pressure to a tight muscle without considering the physiological context, the nervous system often fights back. The tissue tightens further to protect the area. Conversely, by understanding these physiological loops, therapists can use techniques like reciprocal inhibition to “convince” the nervous system to release tension. This approach transforms a standard massage session into a neuro-modulating intervention. The goal is not to force the body into submission but to restore homeostasis.
The Role of Anatomy in Clinical Assessment
One of the most frequent corrections I make involves palpation. A student might rub the skin over the gluteus medius, believing they are treating the muscle, while in reality, they are barely affecting the deep fascia. Effective massage therapy relies entirely on the precision of palpation, which depends on a clear mental image of what lies beneath the skin.
When working with athletes, I often explain that the pain they feel in the knee is actually a compensatory price they are paying for stiffness in the hip or ankle. A therapist with a strong grasp of functional anatomy knows to look for these kinetic chain connections. For instance, restricted ankle dorsiflexion forces the tibia to rotate internally, stressing the knee. A therapist focusing solely on the knee will fail. However, a therapist who understands the chain will treat the ankle to fix the knee.
This level of assessment separates a spa treatment from a sports medicine treatment. It requires the practitioner to constantly ask questions about joint anatomy and movement limitations. Is the restriction articular, muscular, or neural?
How We Teach Applied Body Mechanics
At RSM, we approach the learning process differently. We do not just hand out a trail guide and expect rote memorization. We integrate applied anatomy directly into deep tissue massage techniques. When learning a stroke, the student learns exactly which fiber direction they are engaging and what layer of depth is required.
We utilize a specific pedagogical method:
- Visualization: Using a high-quality anatomy model to see the structure in 3D.
- Palpation: Locating the structure on a living body to feel its texture.
- Action: Asking the client to engage the muscle to confirm location.
- Treatment: Applying the specific massage therapy technique suited for that tissue.
This sequence ensures that students build a tactile library of “normal” versus “dysfunctional” tissue. Over time, their hands become intelligent diagnostic tools.
Ongoing Study in Massage Therapy
The field of sports medicine is not static. New research constantly reshapes our understanding of fascia and biomechanics. Therefore, a therapist’s education cannot end upon graduation. We often see experienced therapists return to our programs to update their foundational knowledge. They may need to unlearn outdated concepts, such as the idea that the IT band can be “stretched”, and replace them with evidence-based protocols.
Massage therapy is a powerful tool, but it is a blunt instrument without the guidance of anatomical science. Whether treating a professional athlete or a general client, the underlying mechanics remain the same. By mastering the body system, therapists become architects of recovery. Ultimately, the best guide is the human body itself, which tells you exactly what is wrong if you have the knowledge to listen.
Exploring Massage Therapy Career Options for the Serious Practitioner

Professional massage training course
The Modern Massage Landscape
Potential students often view the industry through too narrow a lens, assuming the profession is limited to spa environments. This misconception overlooks the rapid integration of manual therapy into mainstream healthcare. In my experience training practitioners at RSM Massage School in Thailand, I have observed that the most successful graduates are those who recognize early on that massage is a clinical tool, not just a luxury service.
The demand for skilled massage therapists has evolved significantly. Patients seeking pain relief for conditions like sciatica or frozen shoulder require a therapist who understands functional anatomy. Consequently, the work environment for modern practitioners has shifted from purely aesthetic settings to multidisciplinary clinics. This shift changes the trajectory of a career. When a therapist can demonstrate that their treatments resolve pathology rather than merely soothing symptoms, they unlock a tier of employment that offers greater stability.
To fully explore the potential of this field, one must look at the specific sectors where manual therapy is currently thriving. The options are vast, but they require distinct skill sets. A job in a palliative care unit demands a different approach than a position with a professional football team. Therefore, understanding the nuances of these environments is the first step in defining a viable career path.
Medical Massage and Therapy Career Pathways
One of the most rapidly growing sectors is the clinical environment. Here, massage therapy functions as a complementary component to orthopedic and rehabilitative care. In this setting, the therapist operates alongside physical therapists and osteopaths. This collaborative dynamic forces the therapist to adopt a medical vocabulary and a deeper understanding of pathology.
Medical massage specifically targets diagnosed conditions. Unlike general wellness sessions, these treatments follow a specific care plan devised to improve range of motion. Therapy in this context is result-oriented. For example, when treating a client with lateral epicondylitis (tennis elbow), the therapist must understand that the pain often originates from extensor muscle overload in the forearm, rather than just local inflammation.
Choosing this occupation path requires rigorous education. Massage schools that focus solely on Swedish massage rarely provide the depth of knowledge necessary for clinical work. Licensed massage therapists in medical settings must be proficient in orthopedic testing and nerve mobilization. The job outlook for clinical therapists is generally stronger than for generalists because patients and providers increasingly seek non-pharmacological pain management solutions.
Work Environments for Massage Therapists
At RSM International Academy, we specialize in sports medicine because it represents the pinnacle of functional manual therapy. Working in sports is demanding and requires the therapist to think critically about biomechanics. When an athlete presents with hamstring tightness, a standard therapist might simply rub the hamstring. In contrast, a sports-focused therapist analyzes the pelvic tilt and assesses lumbar mobility.
The environment in sports medicine is fast-paced. Massage therapists in this sector often travel with teams or work on the sidelines. The work involves pre-event preparation to prime the nervous system and post-event recovery to flush metabolic waste. This is a highly competitive career sector. Success here depends on the ability to deliver immediate, tangible results.
Athletes view their bodies as performance machines. If a therapist cannot explain the causal link between a treatment and improved performance, they will lose the client. Therapy careers in sports medicine often lead to high-profile opportunities, but they also carry higher expectations regarding liability and professional conduct.
Business Options vs. Job Stability
A critical decision for every practitioner is whether to seek employment or start a private business. Both career options have distinct advantages.
Employment offers stability. Working for a franchise or a medical clinic provides a steady stream of clients, handled administrative tasks, and predictable income. For new graduates, this is often the safest route to gain experience. However, the trade-off is often a lower per-hour salary compared to what self-employed therapists charge.
Conversely, private practice allows for total autonomy. A self-employed therapist sets their own rates and chooses their clients. This path appeals to those with an entrepreneurial spirit. However, it requires significant non-clinical work, such as marketing and legal compliance. In my observation, the highest earners are typically those who specialize in a niche area such as sports recovery, and run their own specialized services. They build a reputation for solving difficult cases, which allows them to command higher fees.
Wage Statistics and Job Outlook
When analyzing wage statistics and employment projections, it is vital to look beyond the averages. Government data often lumps all practitioners together, from entry-level spa workers to elite sports therapists. This aggregation can skew the perceived potential of the profession.
General occupational outlook data suggests that the field is growing faster than average. This growth is driven by an increased public awareness of the benefits of therapy. However, the salary range is wide. Entry-level positions in chain spas often pay near minimum wage. In contrast, occupational specialists in medical or sports settings can earn significantly more.
The job outlook is particularly robust for those with advanced certifications. As healthcare providers increasingly refer patients for manual therapy, insurance reimbursement is becoming more common. Projected growth is highest in metropolitan areas where integrative health centers are becoming the norm.
Determining Your Career Path and Finding Jobs
The foundation of a successful massage career is education. The curriculum a student chooses dictates their future options. Many generic programs focus on meeting minimum licensure requirements. While this allows a student to legally work, it often leaves them unprepared for complex clinical cases.
At RSM, we emphasize that education does not stop at graduation. Therapists who rely on outdated modalities eventually stagnate. Those who continue to explore new techniques and scientific findings maintain a competitive edge. Advanced training also protects the therapist’s own body. Poor body mechanics lead to injury and burnout. High-quality education teaches therapists how to use leverage to deliver deep pressure without compromising their own joints.
Integrating into the broader healthcare system presents specific challenges for finding jobs. Medical massage practitioners must navigate the complexities of patient documentation and inter-professional communication. A doctor referring a patient expects a SOAP note using standard medical terminology. If a therapist describes a session using vague language, they lose credibility. However, if they describe the treatment in terms of reducing hypertonicity to alleviate pelvic obliquity, they establish themselves as a peer.
Services provided in a healthcare setting are scrutinized for efficacy. Patients are often there because they are in pain, not because they want to relax. This changes the dynamic of the client-therapist relationship. Empathy remains crucial, but clinical competence takes precedence.
Entering the field of manual therapy is a commitment to lifelong learning. The options available today are far more diverse than they were twenty years ago. From the sidelines of professional sports to the quiet focus of a rehabilitation clinic, the role of the therapist has expanded. By choosing the right education, understanding the market dynamics, and treating the profession with the seriousness it deserves, new practitioners can build a rewarding and sustainable career. The key is to never stop analyzing and never underestimate the profound impact of skilled touch on the human body.
Analyzing the Physiological Benefits of Deep Tissue Massage

Deep Tissue Massage Course for posture correction
While teaching RSM's Deep Tissue Massage Course, I often notice that students over-rely on increasing force to address chronic pain. They assume that if the client feels pain, the therapy is working. In reality, effective deep tissue massage is not about how hard you push; it is about how precisely you engage the anatomical layers.
When we strip away the spa-like generalizations, the benefits of deep tissue massage reveal themselves as a sophisticated interaction between mechanical manipulation and neurological response. My experience in sports medicine has taught me that pain in a specific muscle belly is often just the symptom of a silent, rigid adhesion in the surrounding fascia. Consequently, to truly resolve the issue, a therapist must visualize the three-dimensional architecture of the body.
Analyzing the Clinical Benefits of Deep Tissue Massage
The primary goal of deep tissue massage is to restore the structural integrity of the musculoskeletal system. Unlike relaxation-based modalities, this form of massage focuses on realigning the deeper layers of muscle and connective tissue. When a massage therapist applies sustained pressure to these layers, they are mechanically shearing the cross-links that form between muscle fibers.
In a healthy state, muscles and fascia glide effortlessly over one another. However, chronic stress and repetitive strain cause these layers to adhere, creating a rigid environment where nutrients cannot enter. This ischemia (lack of blood flow) sensitizes nociceptors; the nerves that detect pain. Deep tissue massage intervenes by physically separating these adhered layers. This mechanical separation restores the glide potential of the tissue, allowing the muscle to contract without restriction.
How Deep Tissue Massage Remodels Fibrotic Tissue
In our curriculum, we emphasize that tissue is a dynamic variable. When the body sustains stress or injury, it lays down collagen fibers in a haphazard pattern to patch the area, forming fibrosis or scar tissue. While protective, an excess of fibrotic tissue restricts mobility.
Deep tissue massage acts as a remodeling force. The slow, concentrated strokes introduce a controlled micro-trauma to these fibrotic areas. This stimulus signals the body to break down disorganized collagen and replace it with pliable, linear fibers. Specifically, we often see this in the lateral thigh fascia. By engaging the deep interface between the quadriceps and hamstrings, the massage therapist can free the lateral chain, leading to reduced tension on the knee joint.
The Science of Deep Pressure and Massage Mechanics
There is a precise science to how deep pressure influences the nervous system. A common misconception is that deep tissue massage must be excruciating. This is false. If the pressure is too aggressive, the client’s body enters a sympathetic “fight or flight” state, causing muscles to guard.
Instead, effective deep tissue work operates on the “edge” of resistance. The therapist sinks into the tissue until they meet the barrier. At this depth, the pressure stimulates mechanoreceptors which lower sympathetic tone. This triggers a parasympathetic response, signaling the brain to drop tension levels. Consequently, the massage becomes a dialogue between the practitioner and the client’s nervous system. The release is neurophysiological, not just mechanical.
Differentiating Deep Tissue Protocols
It is important to clarify the distinction between deep tissue massage and Swedish massage. Swedish massage primarily aims to promote relaxation using long, gliding strokes. In contrast, deep tissue massage is corrective.
We utilize specific techniques to address dysfunction:
- Stripping: Deep gliding along muscle fibers.
- Friction: Pressure across the grain to break adhesions.
- Myofascial Release: Sustained pressure to release fascia.
Because the focus is on the deep structure, the massage therapist uses stronger levers, forearms and elbows, to apply consistent force without fatigue. This allows for the manipulation of dense tissue layers that standard massage cannot reach.
Deep Tissue Massage for Chronic Pain and Tissue Recovery
Chronic pain is often the cumulative debt of unresolved dysfunction. Patients with conditions like plantar fasciitis or lower back pain often find standard treatments insufficient because the source lies in the deeper strata of the soft tissue. Deep tissue massage addresses this via the “Pain Gate Theory.” By stimulating sensory fibers with non-noxious pressure, we block pain signals, providing a window of pain relief.
Furthermore, this therapy is essential for muscle recovery following exertion. Athletes accumulate metabolic byproducts like lactate. Tight muscles trap these fluids, leading to soreness. Deep tissue massage acts as a mechanical pump, flushing out stagnant fluid from the interstitial spaces. This exchange accelerates recovery and helps reduce pain associated with stiffness.
Overcoming Ischemia to Improve Circulation
Circulation is the lifeblood of tissue health. Ischemia contributes to degeneration. Deep tissue massage reverses this state. By manipulating deep muscle bellies, we mechanically dilate blood vessels, leading to hyperemia.
This ability to improve circulation extends beyond the local area. The systemic increase in blood flow lowers vascular resistance. For clients with tension headaches, relieving tension in the suboccipital muscles through deep tissue work restores cranial circulation, offering immediate health benefits.
Integrating Massage Therapy into Rehabilitation
At RSM International Academy, we teach that massage therapy is a potent tool within rehabilitation. When a client is recovering from injury, deep tissue massage prepares the tissue for strengthening. You cannot strengthen a muscle inhibited by trigger points.
The therapist plays a crucial role in breaking the pain-spasm-pain cycle. By carefully relaxing muscle spasms, we reduce inflammation markers locally. We also utilize lymphatic drainage techniques within deep tissue protocols to clear inflammatory mediators. This sets the stage for effective physical therapy.
Frequency of Sessions and Safety
For long-term improvement, consistency is key. Deep tissue massage is cumulative. One session may release superficial tension, but deep holding patterns require repeated inputs. We recommend a series of massage sessions to break the pattern of dysfunction.
However, safety is paramount. We do not apply deep pressure over acute inflammation or open wounds. A skilled therapist knows when to back off. The goal is to aid recovery, not induce injury.
The Corrective Power of Manual Therapy
The effectiveness of this modality lies in its specificity. It is a surgical approach to soft tissue dysfunction. Through improved circulation, the breakdown of scar tissue, and neurological resetting, deep tissue massage offers a pathway out of chronic pain.
For those training to become therapists, remember: your understanding of the tissue is your true power. When you combine anatomical knowledge with the skilled application of deep tissue massage, you do not just relax your client, you rebuild them.
Key Takeaways
- Precision: Effective deep tissue massage targets specific layers.
- Hydration: Water supports the metabolic flush after massage sessions.
- Consistency: Chronic pain requires consistent massage work to resolve.
- Health: Deep tissue work supports overall health and performance.
At RSM International Academy, we believe that deep tissue massage, when performed with clinical expertise, is one of the most powerful methods available for maintaining physical health.
Balancing Theory and Practical Learning in Advanced Massage Therapy
Manual therapy and sports medicine massage
Anatomy is often understood in the static sense found in textbooks, which overlooks its critical role in dynamic movement and injury rehabilitation. Students who have memorized anatomical terms usually lack the tactile understanding of the true mechanical origins of pathology. At RSM Massage School here in Chiang Mai, we emphasize that physiological concepts are not just abstract definitions; they are dynamic variables that change based on load, posture, and tissue quality.
To truly master sports medicine-based massage, a therapist must move beyond simple memorization and start visualizing the three-dimensional relationship between structure and function. We do not view the classroom and the treatment table as separate entities. Instead, we treat them as a feedback loop where intellectual understanding drives manual precision, and tactile feedback refines intellectual models.
The Disconnect Between Theoretical Knowledge and Real Application
In traditional massage schooling, there is often a rigid separation between lecture and clinic. Students absorb theoretical knowledge regarding muscle origins and insertions to pass a written exam. Later, they enter a practical module to learn a set routine. This segmentation creates a dangerous gap. A student may know that the sciatic nerve is near the piriformis, but when a client presents with deep gluteal pain, they often fail to differentiate between pathologies because they haven’t learned to translate that knowledge into their hands.
This disconnect leads to generic treatments. If a therapist cannot translate their understanding of pathophysiology into their touch, they default to “rubbing where it hurts.” In sports medicine, this is insufficient. Pain is often a symptom, not the root cause. Without the ability to bridge theoretical concepts with hands-on assessment, the therapist addresses the symptom while the underlying dysfunction remains.
Redefining Education in the Classroom
We approach education differently, believing that teachers must act as clinical guides. In our classroom, a lecture on the lumbar spine does not end with a slide presentation. Immediately following the explanation of the facet joints, we move to the tables to palpate them through the layers of fascia. This method forces the brain to encode information differently, transforming abstract data into sensory data.
This approach requires a specific kind of teacher education. Our instructors are not just delivering content; they are demonstrating how to think like a clinician. By vocalizing their thought process during a demonstration, they model the internal dialogue of problem-solving. This teaches the student to construct their own clinical reasoning pathways, a skill far more valuable than memorization.
Why Practice Must Anchor Abstract Concepts
Intellectual concepts are easily forgotten without a physical anchor. Practice serves as this anchor. When a student reads about the “end-feel” of a joint, it remains a vague idea. It only becomes a clinical tool when they feel the hard stop of elbow extension compared to the firm, springy stop of a healthy knee joint.
We utilize specific practical exercises designed to heighten proprioception and precision. Teaching the depth of pressure required to access the psoas major cannot be learned from a book; it requires repeated, supervised execution. This physical discipline supports the intellectual work. Practical proficiency also involves the therapist’s own body mechanics. A therapist who understands leverage theory but cannot apply it through their own body will be inefficient and prone to injury.
Integrating Research Findings into Daily Treatment
The field of sports medicine is not static, as new research findings constantly challenge old dogmas. For years, static stretching before performance was common practice. However, current research shows that it can temporarily reduce power output. We integrate these updates directly into our practical training, teaching students to evaluate sources critically. This creates a culture of experiential learning where students can test hypotheses in real-time.
The Role of Models in Visualizing Pathology
While hands-on experience is paramount, anatomical models are invaluable for visualizing structures. This is particularly important for deep structures that are inaccessible to direct touch. Theoretical visualization helps prevent injury. If a therapist understands the intricate path of the brachial plexus, they will approach the lateral neck with appropriate caution. We use models to demonstrate these critical areas, ensuring that when a student touches a human body, they are seeing through the layers with their mind’s eye.
Experiential Learning and the Clinical Reasoning Loop
The ultimate goal of combining theory with hands-on work is to develop a therapist capable of independent clinical reasoning. This is a cyclical process we call the Clinical Reasoning Loop.
- Assessment (Theory/Practice): The therapist uses theoretical knowledge of biomechanics to observe movement and practical palpation skills to assess tissue.
- Hypothesis (Theory): Based on the data, the therapist forms a working hypothesis about the root cause of the dysfunction.
- Treatment (Practice): The therapist selects and applies a technique designed to address the hypothesis.
- Re-Assessment (Learning): Immediately after the intervention, the therapist re-tests.
- Adjustment (Synthesis): If the intervention was not successful, the hypothesis was incorrect or the technique was insufficient. The therapist adjusts and begins the loop again.
This loop turns every session into a micro-experiment and is central to our learning philosophy. It elevates the therapist from a technician following a script to a clinician who solves problems. We also provide students with the resources to continue this growth long after graduation, teaching them to build their own case logs and recognize when to refer a client to another specialist.
Bridging the Gap for Elite Therapy
The separation of head and hand is the enemy of mastery in manual therapy. A therapist with brilliant hands but no theoretical grounding cannot adapt to complex injuries. Conversely, an academic with encyclopedic knowledge but poor hands cannot effect change in the tissue.
At RSM International Academy, we recognize that the human body is the ultimate teacher. Our curriculum is designed to give you the language to understand what the body is telling you (theory) and the skills to respond effectively (practice). By rigorously integrating these two domains, we produce therapists who are ready for the demands of elite sports medicine. We train them not just to massage muscles, but to analyze movement, identify dysfunction, and restore performance. This is the only path to achieving true excellence in our field.
Deep Anatomy Knowledge for Orthopedic Massage
Functional Anatomy and Dynamic myofascial release
It's important for us to distinguish between relaxation therapy and clinical remediation. In our sports medicine curriculum, we teach that effective treatment relies on visualizing the three-dimensional machinery beneath the skin. To resolve chronic pain rather than merely masking it, a therapist requires specific anatomy knowledge, and a practical understanding that goes far beyond basic textbook definitions.
Elevating Massage Techniques Through Anatomy
The transition from relaxation-based work to clinical therapy demands a shift in cognitive approach. Standard massage often employs broad, non-specific strokes aimed at general circulation. In contrast, the techniques learned during RSM's Orthopedic Massage Course require pinpoint accuracy. When we treat a client, we are navigating a complex map of the musculoskeletal system.
If a practitioner lacks a deep knowledge of how layers interact, their massage becomes a guessing game. They might press hard on a structure that requires gentle release or stretch a tissue that is already over-lengthened. Consequently, the ability to palpate effectively is directly dependent on the therapist’s mental blueprint of anatomy. This understanding allows us to differentiate between a healthy tendon and a fibrotic adhesion, ensuring that every stroke has a clear therapeutic intent.
Precision in the Shoulder and Upper Limb
To illustrate the importance of this knowledge, consider the shoulder and arm. This region is dense with neurovascular structures, making precise muscle anatomy crucial for both safety and efficacy.
A superficial approach might focus solely on the deltoid muscle when a client reports shoulder pain. However, the deltoid often compensates for deeper dysfunction in the rotator cuff or scapular stabilizers. A therapist must understand these mechanical relationships to restore function.
Moving distally to the elbow, the need for specificity increases. Many massage therapists struggle to differentiate between the structures originating at the medial epicondyle versus the lateral epicondyle.
- Lateral Pain: Often involves the forearm extensor group. Specifically, the extensor carpi radialis brevis is a frequent driver of pathology. However, the brachioradialis muscle also exerts force here. A skilled therapist must palpate the septum between these muscles to release them individually.
- Medial Pain: Conversely, pain at the inner elbow involves the common flexor tendon, where the flexor carpi radialis and ulnaris converge.
- Safety: The cubital fossa (anterior elbow) contains the median nerve and brachial artery. Without precise knowledge of anatomy, a therapist risks compressing these sensitive structures while attempting to treat the distal biceps.
Sustainable Relief and Therapeutic Outcomes
Ultimately, the goal of orthopedic massage is sustainable relief. Clients seek our help because they are in pain or restricted in their movement, and generic approaches have failed them. By grounding our therapy in origins insertions and biomechanics, we offer a logical solution.
When we explain to a client that their elbow pain stems from specific forearm extensor tension, or that their shoulder restriction is linked to scapular mechanics, the treatment becomes educational. This therapeutic partnership encourages the client to trust the process. At RSM, we believe that you cannot fix a machine if you do not understand the blueprint. Therefore, mastering the detailed anatomy of the body is the most critical step in becoming an elite massage practitioner.
The Approach at Our International Massage School in Thailand

Trigger Point therapy and Sports Medicine
A Clinical Perspective on Massage Education
When I established RSM International Academy in Chiang Mai, my objective was to bridge the significant divide between generalized relaxation and clinical therapeutic treatment. In the world of manual therapy, there is an abundance of training focused on sequence memorization. However, memorizing a sequence does not equate to understanding the body. True therapy requires a diagnostic mind. Consequently, we built a curriculum rooted in Dynamic Postural Assessment and science backed sports medicine.
At our massage school here in Thailand, we teach students that the source of pain is rarely where the client points to. It is usually the result of a kinetic chain dysfunction. Consider a client with chronic lower back pain. A standard therapist might apply deep pressure to the lumbar erectors. This often fails because the pain is merely a symptom. In many cases, the root cause lies in a restricted ankle dorsiflexion or a tight iliopsoas. When the psoas shortens, it inhibits the gluteus maximus. As a result, the lumbar extensors overwork to maintain posture, leading to fatigue and pain.
Our training emphasizes this causal logic. We do not simply teach how to rub muscles; we teach how to assess structural integrity. By understanding functional anatomy, a therapist transforms from a service provider into a clinician.
A Scientific Foundation for Clinical Massage
Our methodology is intentionally distinct from the conventional spa models prevalent in Thailand. While relaxation has its place, our mission is to provide an evidence-based education focused on pain relief. We founded this academy on the principles of sports medicine and clinical palpation.
Instead of teaching a generalized routine, we teach a process of assessment and treatment. This style of education requires deep biomechanical knowledge. Students learn to perform orthopedic tests to form a clear clinical picture before beginning hands-on work. This elevates the practice of massage from a generic service to a targeted intervention. The goal is to produce lasting changes in function.
The Difference in Our School Curriculum
The curriculum at RSM is designed for those who seek to elevate their practice. We limit class sizes to ensure every student receives direct feedback. Large classes often result in students mimicking movements without understanding tissue texture. In our courses, tactile sensitivity is prioritized.
We structure our learning environment to focus on:
- Functional Anatomy & Cadaver Study: We go further than standard charts by offering the world’s first massage course with hands-on cadaver palpation training, in collaboration with the Faculty of Medicine at Chiang Mai University.
- Trigger Point Therapy: We teach students to locate taut bands and identify referral patterns. For instance, a headache is often caused by active trigger points in the Sternocleidomastoid (SCM) rather than pathology in the head.
- Deep Tissue Massage & Myofascial Release: True deep tissue massage is about sinking into the fascia, not applying brute force. Our Dynamic Myofascial Release course integrates this with joint mobilization.
This training program is rigorous. It demands that students study outside of practical hours. Because the human body is complex, the learning curve is steep. However, the reward is the ability to resolve chronic pain conditions other therapists have failed to treat.
Advanced Training Beyond a Standard Massage School in Thailand
Standard vocational schools often adhere to curriculums that prioritize safety over efficacy. While our courses are approved by relevant authorities, we view the standard curriculum as a starting point. We push beyond the basics into advanced manual therapies.
Key differentiators include:
- Osteopathic Integration: We incorporate joint mobilization techniques to restore sliding surfaces within the articular capsule.
- Kinetic Chain Assessment: We teach Dynamic Posture Assessment to identify how misaligned movement patterns lead to pain.
- Sports Medicine Protocols: We customize treatments for injury prevention. A runner with shin splints needs a different protocol than a weightlifter with shoulder impingement.
We also focus on longevity. Many careers end due to injury. We teach body mechanics that utilize leverage rather than muscular effort. By stacking the joints and generating force from the core, our students learn to deliver deep pressure for hours without fatigue. This sustainability is crucial for a long-term career in massage education and practice.
To illustrate our depth, consider “Sciatica.” Many clients actually suffer from Pseudo-Sciatica caused by the Gluteus Minimus. Trigger points here refer pain down the leg, mimicking nerve compression. If a therapist treats the spine for a disc issue that doesn’t exist, the client gets no relief. By palpating the Gluteus Minimus, our students reproduce and resolve the pain. This diagnostic accuracy is what defines an international massage specialist.
RSM International Academy is not for those seeking a holiday course. It is for serious practitioners. We provide a massage school experience that challenges the intellect. By focusing on a sports medicine-based approach, we equip graduates to make a profound impact on their clients’ health.
Ergonomics for Sports Massage Professionals: A Sports Medicine Approach

Sports message course
Many massage therapists view ergonomics merely as a set of workplace safety guidelines, overlooking its critical role in the efficiency of force transmission. In my experience training students at RSM International Academy, I often have to explain that the pain a practitioner feels in their lower back or thumb is not just an occupational hazard; it is a sign of a broken kinetic chain. When a therapist generates force solely from their upper body rather than transmitting it from the ground up, they are not only risking injury but also delivering a suboptimal treatment.
To truly master deep tissue and sports massage, a practitioner must move beyond simple memorization of client anatomy and start visualizing the three-dimensional relationship between their own body mechanics and the client’s tissue response. In RSM's Sports Massage Course, we emphasize that the therapist is, in essence, an athlete. Your event is the massage session, and your performance depends entirely on how well you manage your own biomechanical load.
The Biomechanics of the Therapist: Why Posture Failures Occur
In our curriculum, we emphasize that posture is not a static position but a dynamic state of readiness. When a massage therapist stands at the table, they create a closed kinetic chain. The force applied to the client does not originate in the hands; it begins at the feet, travels through the legs, crosses the pelvis, stabilizes through the spine, and finally exits through the contact point.
If any link in this chain is weak or misaligned, the body compensates. Specifically, if a practitioner lacks core stability, the lumbar spine takes the load. This leads to a common error where the therapist tries to “push” into the tissue using triceps strength. This muscular effort creates tension in the therapist’s own trapezius and levator scapulae. Consequently, the client feels a “sharp” pressure rather than a deep, sinking engagement.
Effective mechanics rely on the principle of stacking. By aligning the shoulder, elbow, and wrist directly over the contact point, the skeleton bears the load rather than the muscles. This skeletal stacking allows the therapist to lean their body weight into the stroke, utilizing gravity as a primary energy source. This approach reduces metabolic expenditure and minimizes the risk of burnout.
Analyzing Common Injuries in Massage Therapy
I frequently encounter cases of career-ending injuries labeled as “overuse.” In fact, the problem often begins far from the site of pain. The chain typically starts with a minor mechanical fault, such as working with a high center of gravity. This fault increases torque on the lower back, promotes shoulder elevation, and lays the foundation for chronic inflammation.
The Wrist and Kinetic Chain Failure
One of the most frequent corrections I make is when students attempt to address deep restrictions by solely focusing on thumb pressure. The thumb’s saddle joint is inherently unstable under direct compression. When a massage therapist relies on their thumbs for deep tissue work, they subject a small surface area to massive force.
This mechanical stress often results in De Quervain’s tenosynovitis. In contrast, using the olecranon (elbow) changes the physics of the interaction. By broadening the contact tool, we distribute the force over a larger surface area. Common injuries like carpal tunnel syndrome often stem from working with the wrist in extension. Once the wrist deviates beyond 15 degrees of extension while under load, pressure within the carpal tunnel rises, compressing the median nerve.
Lower Back Pain and the Hip Hinge
The back is perhaps the most vulnerable area for massage therapists. A significant percentage of issues in our field are lumbar strains caused by the “topple” effect. This occurs when a therapist bends at the waist to reach a client on the far side of the table, creating a long lever arm that places immense shear force on the L4 and L5 vertebrae.
To neutralize this ergonomic risk, practitioners must master the hip hinge and the lunge stance. By keeping the spine neutral and bending at the hips and knees, the therapist lowers their center of gravity. This shifts the load from the small erector spinae muscles to the powerful gluteals. At RSM, we integrate this movement pattern into our practice, ensuring that every stroke is powered by the legs.
Optimizing the Massage Table and Equipment Setup
The massage table is the primary workbench of our profession, yet it is often the source of dysfunction. Many therapists set their table height based on visual symmetry rather than biomechanical leverage. A table set too high forces the therapist to elevate their shoulders to generate downward pressure, leading to tension headaches.
Conversely, a table that is too low forces the therapist to flex the lumbar spine to maintain contact. This compromises the core and places the lower back in a vulnerable position. While the standard “fingertip rule” is a good starting point, for deep tissue or sports massage, I often recommend setting the equipment slightly lower. This allows the practitioner to utilize more of their body weight for downward compression without bending the elbows.
Equipment safety also extends to the flooring. Working on a hard surface without shock absorption prevents the feet from making micro-adjustments. This rigidity travels up the chain, locking the knees and hips. Investing in high-quality supportive footwear allows for dynamic footwork, which is essential for transferring weight effectively.
Workplace Posture and Dynamic Movement
Static posture is the enemy of the massage therapist. Standing in one position for an hour-long treatment causes blood pooling in the lower extremities and fatigue in the postural muscles. In our training, we treat the massage session as a dance. The therapist must constantly shift their weight from the back foot to the front foot.
This concept of “dynamic work ergonomics“ implies that the therapist is never truly still. Even during a static compression technique, the therapist should be micro-adjusting their center of gravity. For therapists who perform seated work, a saddle stool can maintain the natural lumbar curve better than a flat chair. The saddle shape forces the hips into an open angle, reducing the tendency to slouch.
Identifying Ergonomic Hazards and Corrective Practice
Ergonomic hazards are not limited to the physical mechanics of the session. The “invisible” load of the profession, scheduling and mental focus, plays a massive role in injury rates. Massage tasks that require repetitive high-force output deplete glycogen stores and fatigue the nervous system. When the nervous system is fatigued, proprioception degrades, leading to sloppy mechanics late in the day.
We advise our students to structure their day with “active recovery” blocks to prevent repetitive strain on specific muscle groups. Ultimately, the longevity of a massage therapist depends on their commitment to self-care. At RSM International Academy, we do not view self-care as a luxury; it is a professional responsibility. If your neck is stiff or your health is compromised, your ability to palpate tissue restrictions is diminished.
We recommend a daily practice of corrective exercises designed to reverse the postures of the workplace:
- Thoracic Extension: Reversing the kyphotic curve developed from looking down at clients.
- Forearm Stretching: Releasing tension in the flexor compartment.
- Gluteal Activation: Ensuring the glutes remain the primary drivers of force.
By treating our own bodies with the same level of clinical rigor that we apply to our clients, we ensure that we can continue to practice this demanding craft for decades. By respecting the laws of biomechanics and recognizing the risk factors inherent in our trade, we elevate the standard of care for everyone.
Shiatsu Acupressure Points Explained by a Sport Medicine Teacher

Hironori with USA Paralympic National Team Trainer
Many students initially view shiatsu as purely energetic. They memorize locations without understanding the underlying tissues. However, my experience in sports medicine suggests that this approach limits efficacy. When we analyze the classical locations of these targets, we almost invariably find that they correspond to motor points, neurovascular bundles, or areas of dense fascial convergence.
The “magic” of acupressure is not in the chart, but in the application. It lies in understanding how pressure applied to specific coordinates influences the nervous system and alters muscle tone. RSM's Shiatsu Massage Course bridges the gap between traditional wisdom and modern anatomical science.
The Science Behind Acupressure Massage
While traditional texts explain acupressure through the movement of Qi (life energy), modern sports medicine offers a physiological parallel crucial for the evidence-based therapist. When we stimulate specific areas, we engage in mechanotransduction. This is the process by which cells convert mechanical stimulus into biochemical activity.
The concept of meridians aligns remarkably well with what Thomas Myers describes as “Anatomy Trains” or myofascial kinetic chains. For example, the Urinary Bladder meridian runs parallel to the Superficial Back Line. A restriction in the plantar fascia often transmits tension up to the sub-occipital region.
Treating these pathways is not just about balancing abstract energy; it is about releasing fascial adhesions that compromise movement efficiency. Consequently, effective acupressure massage does more than relax a client. It restores the glide between tissue layers. By targeting high-resistance areas along these chains, we reduce mechanical drag on the musculoskeletal system, leading to improved range of motion and a reduction in compensatory patterns.
Defining Pressure Points and Tsubos
In the Japanese tradition, the specific locations we treat are called “Tsubos.” A Tsubo is often described as a vessel where tension accumulates. Clinically, these spots are rarely random. A skilled palpation assessment usually reveals that a Tsubo corresponds to a trigger point or a myofascial adherence.
Pressure points are areas of high electrical conductivity and lower skin resistance compared to the surrounding tissue. When a therapist applies perpendicular force to these areas, several physiological responses occur:
- Ischemic Compression: Temporary restriction of blood flow causes a reactive hyperemia upon release, flushing out metabolic waste products like lactic acid.
- Neurological Gating: Strong, non-painful stimulation of large sensory fibers blocks the transmission of pain signals from smaller fibers at the spinal cord level.
- Autonomic Switching: Sustained, deep pressure stimulates the vagus nerve, shifting the body from a sympathetic state to a parasympathetic state.
Understanding this biology changes the intent of the treatment. We are communicating with the central nervous system to downregulate pain signals and reset muscle tone.
Mastering Shiatsu Technique
The defining characteristic of shiatsu is the quality of touch. Unlike other forms of massage that utilize friction, this modality relies on static, perpendicular penetration. The Japanese term literally translates to “finger pressure,” but the technique requires the use of the whole body’s weight, not just the strength of the thumb.
Many therapists fail because they use muscle strength to push, resulting in a “poking” sensation. Conversely, correct shiatsu technique involves stacking the joints—shoulder over elbow, elbow over wrist—and leaning body weight into the recipient.
This static pressure allows the tissue to melt. When we apply a rubbing motion, the muscle spindle fibers often react by contracting. By keeping the hand pressure stable, we bypass this stretch reflex. The nervous system accepts the intrusion, allowing access to deeper layers without eliciting a defensive guarding response.
Mapping Specific Acupoints to Anatomy
At RSM, we train students to locate points via palpation rather than visual measurement alone. However, knowing the anatomical correlation is essential. Here, we analyze key acupressure points used in sports recovery.
GB21 (Jian Jing)
Located at the highest point of the shoulder.
- Anatomical Correlate: Direct access to the upper trapezius belly and supraspinatus.
- Clinical Application: A primary target for tension headaches. In overhead athletes, the upper trapezius often becomes dominant. Releasing GB21 helps restore scapular mechanics.
- Caution: This area contains the lung apex. While deep needle insertion in acupuncture carries risks, manual pressure is generally safe.
LI4 (He Gu)
Located on the dorsum of the hand, between the first and second metacarpals.
- Anatomical Correlate: The first dorsal interosseous muscle and adductor pollicis.
- Clinical Application: Famous for general pain relief. As the distal terminus of the arm lines, releasing high-tone intrinsic hand muscles creates a reflex relaxation effect up the entire arm chain.
ST36 (Zu San Li)
Located four finger-widths below the patella, lateral to the tibial crest.
- Anatomical Correlate: The tibialis anterior muscle.
- Clinical Application: Critical for runners, as the tibialis anterior governs ankle dorsiflexion. Tightness here leads to shin splints. Treating ST36 directly addresses hypertonicity in the anterior compartment.
BL23 (Kidney Shu)
Located in the lumbar region at the L2 level.
- Anatomical Correlate: Accesses the erector spinae and Quadratus Lumborum (QL).
- Clinical Application: The QL is often the culprit in non-specific low back pain. Deep, sustained pressure here releases deep stabilizing muscles that standard surface massage often misses.
Applying Pressure for Clinical Effect
The effectiveness of acupressure depends entirely on the dosage of force. We teach a concept called “sinking.” The therapist makes contact with the skin and waits. As the superficial fascia relaxes, the therapist sinks to the muscle layer, and finally to the depth of the pressure point.
Western medicine often dismisses “Qi” or energy flow. However, if we interpret “blockage of Qi” as “impediment to blood flow,” the concepts align. When a muscle is hypertonic, it compresses vasculature, creating a local hypoxic environment. By releasing these restrictions through points massage, we restore oxygenated blood flow, allowing cellular repair to function optimally.
Furthermore, the modern athlete is often stuck in a state of sympathetic dominance—high stress and constant alertness. Recovery cannot occur in this state. Acupressure is a potent tool for flipping this switch. The rhythmic pressure stimulates proprioceptors, slowing the heart rate and restoring autonomic balance. Without this systemic shift, local tissue work provides only temporary relief.
Integrating Acupressure Techniques
At RSM International Academy, we do not view shiatsu acupressure as a standalone cure-all. Instead, it is a vital component of a comprehensive rehabilitation strategy. A therapist might use these techniques to release a hypertonic antagonistic muscle before asking the client to perform a strengthening exercise.
For instance, if a client has limited knee extension due to tight hamstrings, stretching alone may trigger the stretch reflex. Applying pressure to the hamstring acupoints first downregulates the tone. This creates a neurological window where the muscle is more compliant, making subsequent mobility work significantly more effective.
The study of shiatsu acupressure provides a map to the body’s most influential neuromuscular junctions. By understanding the anatomy under the points, the physiology of pressure, and the mechanics of the kinetic chain, a therapist transforms a simple treatment into a targeted medical intervention. Whether addressing chronic pain or acute tightness, we locate the restriction, apply precise force, and wait for the nervous system to respond. This fusion of ancient technique and modern science defines our standard of care.
Integrated Deep Hip Rotator System and Femoral Head Centration

Functional Assessment of Hip Joint Mobility
The piriformis, superior gemellus, obturator internus, and inferior gemellus function as a single integrated unit rather than as isolated muscles.They share a common insertional system and work together to control deep hip stability.
Among them, the obturator internus plays a specialized role. Its tendon-dominant, dense, and blade-like structure is designed primarily for tension regulation rather than force production.
The superior and inferior gemelli act as dynamic stabilizers, guiding and modulating the tension of the obturator internus tendon as it changes direction around the pelvis.
Through this coordinated system, the deep external rotators are responsible for precise femoral head centralization, ensuring optimal hip joint centration during movement and load transfer.
This mechanism explains why isolated activation of a single muscle is functionally unrealistic, and why dysfunction within this system should be understood as a unit-based coordination failure, not an individual muscle problem.
The Clinical Benefits of Remedial Massage Training
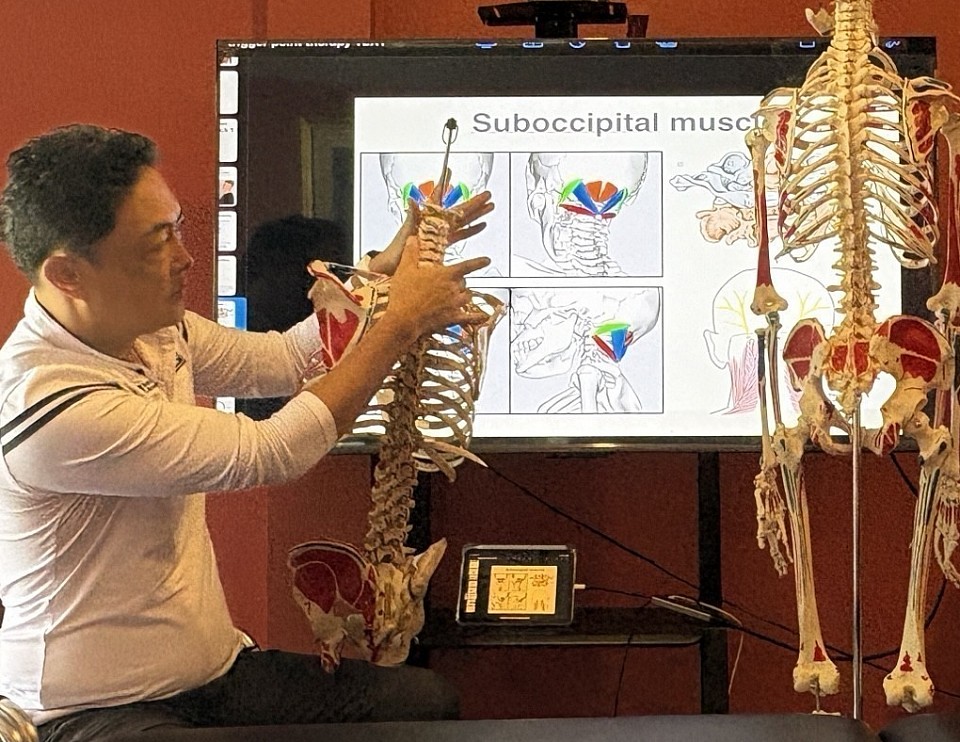
Remedial Massage Course
Many therapists view their initial education as a static foundation, overlooking the critical role that advanced diagnostic skills play in long-term treatment success. One of the most frequent corrections I make during practical training in RSM's Remedial Massage Course is when students attempt to address pain by solely focusing on the site of symptoms. In my experience, the pain a client feels in their lower back is often a compensatory price they are paying for stiffness in the hip or restriction in the ankle. This distinction between treating symptoms and identifying root causes is what defines the transition from a standard therapist to a clinical practitioner.
To truly master this field, a therapist must move beyond simple memorization of anatomical points. They must visualize the three-dimensional relationship between musculoskeletal structures. This is where the specific education provided in remedial courses becomes essential. It shifts the focus from general relaxation to targeted rehabilitation.
Moving Beyond Relaxation: The Remedial Difference
General massage often prioritizes the parasympathetic nervous system response—relaxation. While valuable, this approach often fails to resolve mechanical dysfunctions. In contrast, massage therapy grounded in remedial principles operates on a logic of assessment and correction. Students in our program learn that “remedial” implies a remedy; it is a solution-oriented modality designed to reverse dysfunction and restore range of motion.
When a client presents with hypertonicity, a remedial perspective questions why the tension exists. Is it a result of posture or a shortened muscle group? This analytical process distinguishes a massage therapist who merely relieves stress from one who resolves the physiological drivers of that stress.
The Role of Assessments in Injury Prevention
Treatment without assessment is merely guessing. Effective injury prevention relies on the ability to detect potential failures in the kinetic chain before they manifest as acute pain. During training, we emphasize Dynamic Postural Assessment. This involves observing a client not just statically, but in motion.
For example, a valgus collapse at the knee often indicates weakness in the gluteus medius. If left unaddressed, this increases shear force on the knee joint. A therapist trained in remedial assessments creates a treatment plan that targets these specific imbalances. Consequently, the therapy session becomes a proactive measure against future injuries, ensuring better long-term health and fitness for the client.
Managing Chronic Conditions and Pain
Chronic conditions such as frozen shoulder or sciatica are rarely the result of a single event. They are usually the accumulation of micro-traumas. Addressing these issues requires a strategic approach that goes beyond basic massage.
Consider “Lower Crossed Syndrome.” This involves tight hip flexors and weak glutes. A standard approach might only massage the sore lower back, providing temporary relief. However, the tight hip flexors will immediately pull the pelvis back into an anterior tilt once the client stands up. Remedial training teaches the therapist to release the antagonist muscles to allow the glutes to fire correctly. As a result, the ability to manage pain effectively hinges on this understanding of biomechanics.
Optimizing Athletic Recovery and Performance
In the world of competitive sports, recovery is as important as training. Athletic recovery strategies in remedial massage focus on flushing lactate and preventing adhesion formation.
When working with an athlete, we often focus on deep fascial compartments to prevent entrapment of nerves. This specialized care supports the athlete’s performance by ensuring their mechanical components are operating without restriction. Furthermore, knowing their body is being fine-tuned by a professional provides significant mental benefits and can help lower stress levels before competition.
Advanced Massage Techniques and Career Growth
The toolbox of a remedial therapist is diverse. Remedial training introduces advanced massage techniques like Myofascial Release (MFR) and Muscle Energy Technique (MET). We use MET to lengthen shortened muscles and mobilize restricted joints by having the client actively contract against a counter-force.
Mastering these techniques requires dedication to continuous education. Graduates with a diploma in remedial massage find themselves in high demand. The career opportunities extend to sports teams, physiotherapy clinics, and rehabilitation centers. The market recognizes that a therapist who can perform an orthopedic assessment is a vital asset.
Summary of Core Competencies
The benefits of this specialized training are tangible. To summarize the core skills gained:
- Advanced Assessment: Analyzing posture and gait to identify the root cause of dysfunction.
- Anatomical Fluency: Deep understanding of origin, insertion, and action of major muscle groups.
- Technique Diversity: Proficiency in MFR, MET, and Trigger Point therapy.
- Clinical Reasoning: Designing massage courses of treatment based on logic rather than routine.
Choosing to specialize in remedial work is a commitment to excellence. It demands more study and practice, but the rewards are clear. Whether helping an athlete return to their sport or helping a client move without pain, the ability to assess, reason, and treat effectively is the true value of remedial massage.
